How do I recognize a stroke and what should I do?
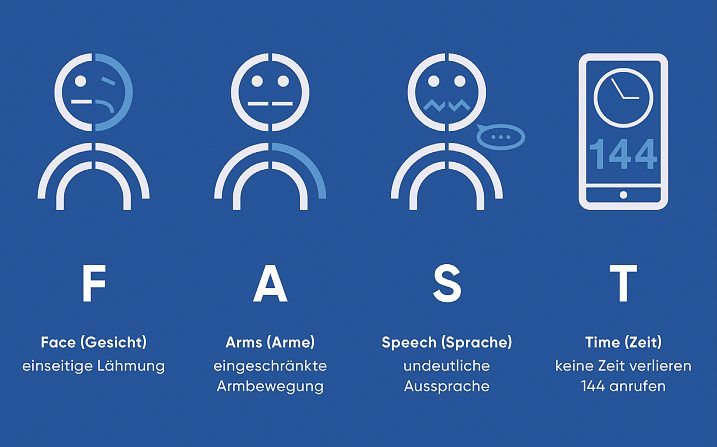
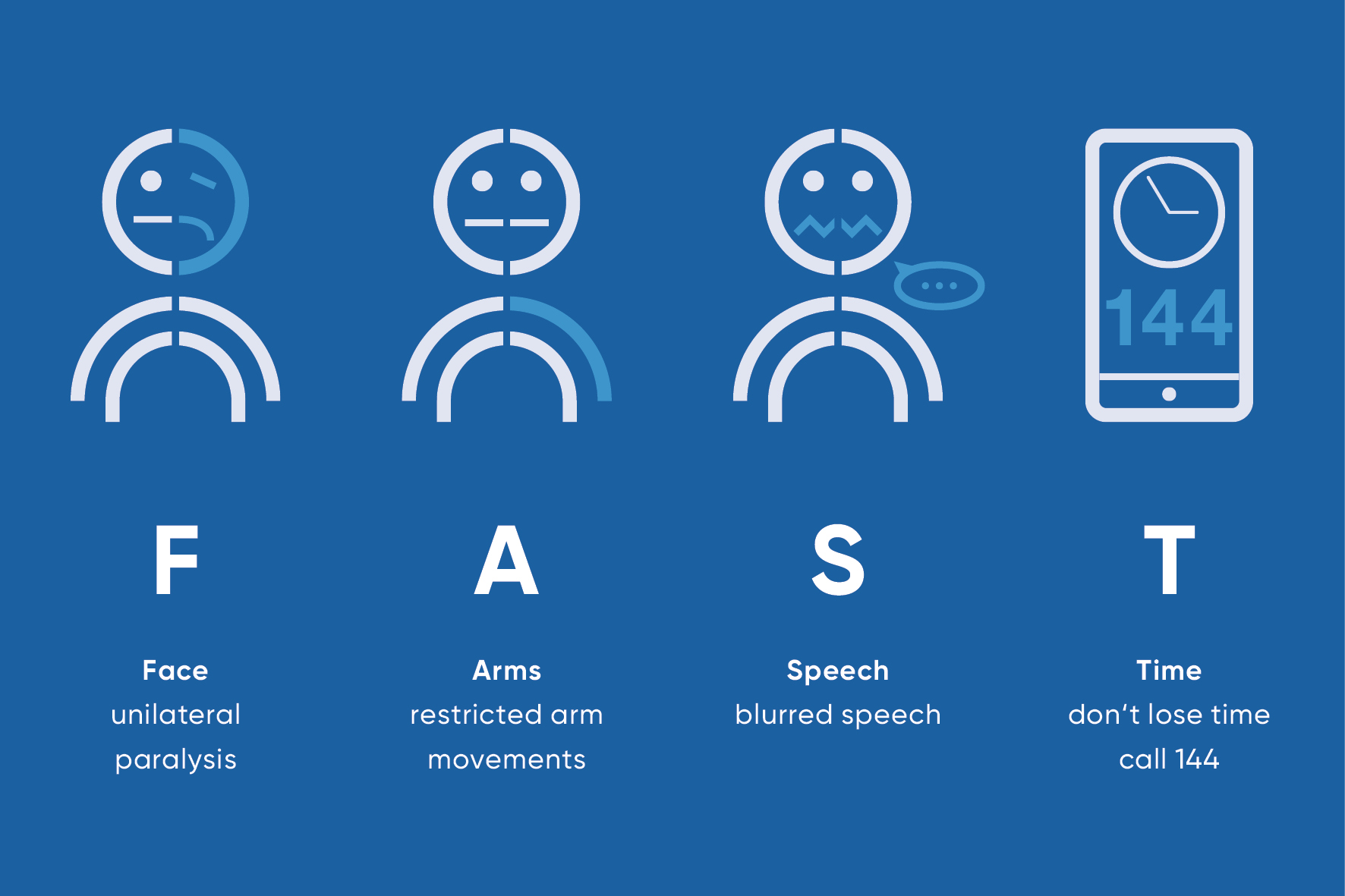
FAST
F – A – S – T stands for Face (face), Arms (arms), Speech (speech) and Time (time).
- Face: Ask the person to smile.
Is the face distorted on one side?
- Arms: Ask the person to stretch their arms forward and turn their palms upwards.
Can the arms be raised? Do they sink or do the palms turn inwards?
- Speech: Have the person repeat a simple sentence.
Is she unable to do this or does her voice sound washed out?
- Time: Call 144 immediately and describe the symptoms and onset of symptoms.
What is a stroke?
There are different types of stroke: an ischemic stroke, i.e. reduced blood flow to the brain, and a hemorrhagic stroke, i.e. a cerebral hemorrhage. Both forms can lead to impairments throughout the body, depending on the area of the brain in which the stroke has occurred. This is because each brain region controls different bodily functions.
What is a stroke?
A stroke often does not announce itself to those affected, but occurs abruptly – like a sudden blow. This is why this dramatic dysfunction in the brain is also known as a stroke. In around 85 percent of cases, it occurs because a blood vessel leading to the brain is blocked; this is known as an ischemic stroke. This results in functional limitations in the affected areas of the body, which can manifest themselves as neurological deficits such as paralysis, speech disorders, dizziness or visual impairment. If the blood vessel is not reopened within a few hours, these disorders can persist. In about 15 percent of cases, however, it is a hemorrhage in the brain: a blood vessel has burst, which increases the pressure in this area; this form is called a hemorrhagic stroke.
Strokes mostly affect older people, around four-fifths of whom are over 60 years old. But younger people, even children, can also have a stroke.
Stroke: causes and risk factors
Both forms of stroke, the more common ischemic stroke and the hemorrhagic stroke, have different causes. It is very important to search thoroughly for the cause of the stroke in order to prevent a recurrence.
Ischemic stroke
In an ischemic stroke, a blood vessel leading to the brain is blocked. As a result, the underlying tissue is more or less cut off from the blood supply, and oxygen and sugar are no longer sufficiently available. If this condition lasts longer, the undersupplied area dies off. In addition to various rare causes, these mechanisms are the main possible causes of vascular congestion:
- Often, arteriosclerosis has been present for years. A blood clot (thrombus) can form at a narrow point in the vessel and block the bloodstream (local thrombotic occlusion) or the blood clot can break loose (embolus) and then block a smaller vessel further distally (=in the direction of blood flow) (arterio-arterial embolism).
- A clot forms in the heart, which then travels via the bloodstream to the brain and blocks a vessel there (cardioembolism). This can occur with cardiac arrhythmias such as atrial fibrillation.
- The smallest blood vessels in the brain are damaged by the long-term influence of risk factors such as high blood pressure or smoking, or by predisposition, and become blocked. This is known as a “microangiopathic” stroke.
- In younger people, other causes play a greater role, for example the so-called “dissection” of the vessels leading to the brain, where a tear can occur within the vessel wall.
Hemorrhagic stroke
The most common cause of a hemorrhagic stroke is high blood pressure. The blood vessels are permanently overloaded by the high blood pressure and can tear. If this happens in the brain, a cerebral hemorrhage occurs. The escaping blood exerts mechanical pressure on the surrounding area. The surrounding nerve cells are damaged. In addition to high blood pressure, there are rare causes of cerebral hemorrhage, such as vascular malformations in the brain.
Risk factors for a stroke
There are various factors that significantly increase the risk of a stroke. You cannot influence two of them. These are:
- Age: Most of those affected are over 60 years old.
- Family predisposition: If one or even several of your relatives have already had a stroke, your own risk may also be increased.
However, there are four times as many other known risk factors for which you can reduce the risk of a stroke yourself with medical support:
- Smoking: Tobacco consumption is one of the most important preventable risk factors.
- High blood pressure (hypertension): Permanently high blood pressure damages the blood vessels and promotes strokes.
- Diabetes mellitus: A poorly controlled blood sugar level can damage the blood vessels and increase the risk.
- Elevated blood lipid levels (e.g. LDL cholesterol): promote hardening of the arteries (atherosclerosis).
- Overweightespecially abdominal fat: severe obesity is associated with other risk factors such as high blood pressure and diabetes.
- Lack of exercise: An inactive lifestyle increases the risk on several levels.
- Excessive alcohol consumption: Regular high alcohol consumption damages blood vessels and organs.
- Chronic stress: Persistent psychosocial stress can have a negative impact on cardiovascular disease.
Symptoms of a stroke
There are a number of signs that can indicate a stroke. These are mostly neurological deficits. The most common symptoms are
- A feeling of weakness (paresis) or total loss of muscle strength (plegia). Typically, these symptoms only occur in one half of the body, as the stroke usually only affects one half of the brain. The opposite side of the body is then affected by the feeling of weakness. Example: The stroke affects the right side of the brain, paresis or plegia occur in the left arm and leg.
- Sensory disturbances such as numbness, affecting one half of the face and one arm
Slurred speech, slurred speech and difficulties with communication show the range of speech and language disorders.
- Dizziness and unsteady gait: This can manifest as a sudden spinning or swaying sensation, accompanied by difficulty maintaining balance, which can lead to an unsteady, staggering gait or even falls.
- Swallowing disorders (dysphagia): Those affected may have difficulty swallowing saliva, liquids or food. This can be manifested by frequent choking, coughing or gagging during or after eating and drinking, or by the feeling that something is stuck in the throat.
- Visual disturbances: These can take many forms, such as suddenly seeing double vision, blurred vision, temporary blindness in one eye or a restricted field of vision (as if part of the visual area is covered
- Confusion: Sudden disorientation. Those affected appear restless and unfocused, can no longer assess situations correctly or answer simple questions adequately.
- Drowsiness to unconsciousness: This can range from severe drowsiness and apathy to a state in which the person no longer reacts to external stimuli. Deep unconsciousness is less common in strokes, but is a very serious sign.
- Very severe, sudden onset of headache and vomiting
The symptoms usually occur suddenly. An exception to this is the so-called wake-up stroke, where those affected wake up in the morning with symptoms. They were therefore unable to notice when exactly they had started, as this happened during sleep.
But it doesn’t matter whether you notice these symptoms from one minute to the next or only in the morning, whether they are dramatic or mild: You should always call the emergency services (144) immediately or have them call you. Because every minute counts when treating a stroke. A stroke can be life-threatening. And the more time that passes before treatment begins, the greater the risk of permanent damage.
Stroke: Diagnosis with us
In the event of neurological deficits, the ambulance service usually takes the patient immediately to a specialized center (stroke unit, stroke center). As a stroke center, the USZ offers all the possibilities of modern stroke care at any time of day or night. Specialists from neurology, neuroradiology and neurosurgery work closely together on an interdisciplinary basis. Other hospitals with a stroke unit carry out the necessary diagnostics and transfer patients to the stroke center if necessary. The diagnosis must be made very quickly and consists of a neurological examination to clarify the symptoms in more detail: Computed tomography or MRI. The CT scan helps to determine whether it is ischemia or a cerebral hemorrhage, i.e. whether a blood vessel is blocked or has burst. This distinction is important because the acute treatment of these two forms of stroke is very different.
In the further course, the cause of the stroke must then be clarified with the help of:
- Ultrasound examination of the neck vessels
- Ultrasound examination of the heart
- Cardiac waveform (over at least 48 hours) to detect whether cardiac arrhythmia is present.
Stroke: gender-specific aspects
Although the classic signs of a stroke – such as sudden paralysis on one side, speech disorders or loss of vision – generally apply to all genders, there are important gender-specific differences in both the symptoms and the risk factors that need to be taken into account in women. Awareness of these differences is crucial as they can influence timely diagnosis and treatment.
Differences in symptoms are rare. However, as women often suffer a stroke at an older age and are then more likely to live alone, symptoms can be less specific.
It is important to emphasize that women can also suffer the classic symptoms, and overall are even more likely to suffer a stroke than men.
Special risk factors for women
Women have some gender-specific risk factors for stroke, and certain common risk factors may put them at a higher relative risk:
- Hormonal factors: Taking the oestrogen-containing contraceptive pill (especially in combination with smoking), pregnancy (and complications such as pre-eclampsia) and hormone replacement therapy during the menopause can increase the risk.
- Atrial fibrillation: This cardiac arrhythmia is associated with a higher risk of stroke in women and is often more severe than in men.
- Diabetes mellitus: Women with diabetes tend to have a higher risk of stroke than men with diabetes.
- Migraine with aura: This type of migraine affects women more frequently and is a known risk factor for ischemic strokes.
- Older age of onset: On average, women often suffer strokes at an older age than men, which can be associated with an increase in other comorbidities and a potentially more complex initial situation.
Knowledge of these gender-specific differences is of great importance both for prevention and for responding quickly and correctly in an emergency in order to optimize treatment outcomes for all those affected.
Stroke care at any time of day or night
The USZ offers all the possibilities of modern stroke care at any time of day or night. Specialists from neurology, neuroradiology and neurosurgery work in three shifts to achieve this. This ensures high-quality care even at night and at weekends. The Stroke Center at the USZ is very active in research, both in the network of all stroke specialists in Switzerland and with its own studies on therapies in acute treatment and rehabilitation. At the USZ, you will find the right specialist for every stroke-related problem in an emergency and long after the acute phase.
Preventing and recognizing strokes at an early stage
The risk of a stroke can be reduced if you control and treat the common risk factors in particular. We can advise and help you with this as part of our specialized stroke consultation hours:
- Adjust elevated blood pressure well. We support you in lowering your blood pressure through the right dose of medication and a healthy lifestyle.
- Protect yourself from high blood lipids or sugar levels with a healthy diet, exercise and, if necessary, medication, which we will work with you to optimize.
- Stop smoking. We will help you to find support.
- Make sure you exercise regularly. Activity is at least as important as losing weight if you are overweight. Find an activity that you enjoy.
- If you sometimes have palpitations or other pulse irregularities, please have them checked by a cardiologist.
- Avoid stress. We will be happy to help you find ways to do this.
In addition, an ultrasound examination of the blood vessels, such as the carotid artery, can show whether the blood vessels are in good condition or whether the innermost layer of the vessel wall has changed – an important indication of arteriosclerosis. Of course, regular blood pressure checks complement the stroke prevention program.
Course and prognosis of a stroke
A stroke can be life-threatening. In industrialized nations such as Switzerland, stroke is the third leading cause of death. It can lead to lifelong disabilities, but also to dementia. This results in enormous costs for the healthcare system (direct healthcare costs alone amount to over CHF 700 million per year).
A stroke is always a medical emergency and treatment should start as soon as possible. Every minute counts. If therapy is started as soon as the first symptoms appear and only a small area of the brain is affected, the stroke can, in the best case scenario, have no consequences.
Unfortunately, sometimes the therapy does not work quite as quickly, and more or less impairing functional disorders remain – such as speech disorders and partial paralysis. However, with the appropriate neurorehabilitation, these can disappear or at least be alleviated over time. The brain develops the ability for intact areas to learn and take over the tasks that were lost with the damaged areas. However, this often requires a lot of time, but also the strength, will and motivation of those affected.
Self-help groups
The exchange with people who are affected by the same disease can be a great support in coping with the disease. Advice on finding a suitable self-help group is available from Selbsthilfe Zürich and Fragile Suisse. Self-Help Zurich and the University Hospital Zurich are cooperation partners in the national project “Health literacy thanks to self-help-friendly hospitals”. We can help you find the right support in our consultation hours.
Stroke treatment
Depending on whether it is an ischemic stroke (caused by a blocked blood vessel) or a hemorrhagic stroke (caused by a cerebral hemorrhage), the therapies differ fundamentally. In each individual case, however, the time factor is absolutely critical. Immediate, precise diagnosis, usually by means of imaging procedures such as computer tomography (CT) or magnetic resonance imaging (MRI), is therefore essential. This makes it possible to quickly identify the type of stroke and thus initiate the appropriate, often very different, acute treatment without delay.
In the case of an ischemic stroke, the main aim is to restore the blood supply to the affected area of the brain as quickly as possible (reperfusion). This can be done with medication by dissolving the blood clot (systemic thrombolysis) or mechanically by removing it using a catheter procedure (thrombectomy). At the USZ, we switched to the modern lysis drug tenecteplase in March 2026 (link to USZ web info), which accelerates therapy. Thrombectomy is carried out in close cooperation with our colleagues in interventional neuroradiology (link?) – because here too, the best method is selected for each patient.
In haemorrhagic strokes, on the other hand, the focus of acute therapy is on stopping the bleeding, controlling the often increased intracranial pressure and stabilizing vital functions. This may, for example, require blood pressure regulating measures, the administration of medication for blood clotting or, in certain cases, neurosurgical intervention.
Regardless of the cause, the immediate transfer of the patient to a specialized department (stroke unit or stroke center) is of crucial importance. Continuous monitoring and a rapid response to possible complications can be guaranteed there. However, the primary goal of all these rapid and targeted measures is always to save as much brain tissue as possible, to minimize or restore as much neurological function as possible as a result of the stroke and to set the course for subsequent rehabilitation and secondary prevention at an early stage
Stroke: aftercare and long-term care
Aftercare following a stroke is a central component of treatment and begins during the hospital stay. The aim is to prevent a recurrence of stroke, minimize consequential damage and promote independence.
Depending on the severity of the neurological deficits, acute treatment is followed by inpatient or outpatient neurorehabilitation. This can include physiotherapy, occupational therapy, speech therapy and neuropsychological care and is individually tailored to the needs of those affected.
Another important focus of aftercare is secondary prevention. This includes finding and treating the cause of the stroke, consistent treatment of risk factors such as high blood pressure, diabetes mellitus, elevated blood lipid levels or cardiac arrhythmia, as well as long-term drug therapy. Regular medical check-ups help to adapt the treatment optimally.
We offer an interdisciplinary neurovascular board for those affected by vascular diseases, such as narrowing (stenosis) of vessels, where we discuss cases together with specialists from the Department of Neurosurgery and Neuroradiology and suggest a therapy. This can also be carried out on external referral from a neurologist or general practitioner. This ensures that the entire expertise of the Neurocenter is available to those affected. In our joint interdisciplinary cerebrovascular consultation (ICS), we can discuss these decisions with you or arrange for further diagnostics.
Psychosocial aspects also play an important role after a stroke. The physical and emotional consequences of a stroke place a heavy burden on many sufferers and their relatives. Counseling, psychosocial support and exchanges in self-help groups can help people to cope better with everyday life. At the University Hospital Zurich, interdisciplinary teams provide patients with comprehensive, long-term support even after the acute phase – with the aim of maintaining their quality of life, independence and safety in the best possible way.
FAQ on the subject of strokes
A stroke is the generic term for a sudden circulatory disorder in the brain. A cerebral hemorrhage is a form of stroke in which a blood vessel in the brain bursts; the other main form is ischemic stroke, caused by a blocked blood vessel.
The first signs usually occur suddenly and can be weakness or paralysis on one side (face, arm, leg), speech or comprehension difficulties, sudden visual disturbances (often in one eye), dizziness with unsteady gait or very severe, unusual headaches. Use the FAST test (Face, Arms, Speech, Time) to recognize symptoms quickly. Even if you are not sure – it is better to come “too early” than too late.
Many strokes occur without any precursors (“out of nowhere”). Transient ischemic attacks (TIA) can be a precursor to a stroke. These are short-term, stroke-like symptoms (e.g. paralysis, speech disorders) that disappear completely within minutes to hours, but are considered serious warning signs of an impending stroke. Also inform 144 during or after a TIA and seek help in a stroke unit or stroke center.
A stroke itself usually occurs suddenly without much warning. Transient ischemic attacks (TIA) as possible precursors can occur hours, days or weeks before a stroke, but not every person affected experiences such warning signs.
A stroke can manifest itself in the eye through sudden visual disturbances, such as loss of vision in one side of the visual field, seeing double vision, blurred or foggy vision or blindness in one eye. This is also a warning signal and should lead to an immediate emergency presentation.
There is no difference; the terms apoplexy (or apoplexia cerebri) and stroke are used interchangeably. Apoplexy is an older medical term for a sudden circulatory disorder of the brain that is no longer used today.
Chronically high blood pressure (arterial hypertension) is a major risk factor for a stroke. A permanent blood pressure of over 140/90 mmHg significantly increases the risk, with the risk increasing further with rising values; however, there is no exact threshold above which a stroke is an immediate threat, as other individual factors also play a role. If you have high blood pressure, talk to your family doctor and ask for support in adjusting it.
The chances of a full recovery after a stroke depend on many factors, including the severity and location of the stroke, the speed of treatment (“time is brain”) and the quality of rehabilitation. Some people recover completely or with only minor limitations, while others can suffer permanent disabilities.
The three main causes are:
- Atherosclerosis of the large arteries supplying the brain (macroangiopathy): arteriosclerosis leads to narrowing or rupture of plaques with localized clot formation (thrombosis) or carry-over of clot fragments (arterio-arterial embolism).
- Cardiac embolism: Blood clots that form in the heart (often in atrial fibrillation or after a heart attack) and are washed into the brain.
- Disease of the small cerebral vessels (microangiopathy/lacunar infarcts): Damage to small arteries deep in the brain, often caused by chronic high blood pressure or diabetes.