For patients
As a patient, you cannot register directly for a consultation. Please get a referral from your primary care physician, specialist. For questions please use our contact form.
A cochlear implant enables people with severe hearing loss or deafness to hear again - even when hearing aids no longer help. Here you will find information on how it works, the implantation procedure and aftercare.
The sound signal that our ear receives is normally converted into nerve impulses by the hair cells in the cochlea. The sequence of nerve impulses is processed in the brain, creating an auditory impression. If the hair cells are damaged in a hearing loss, signals can no longer be transmitted to the nerve cells. If the auditory nerve is not damaged, it can be stimulated directly via a cochlear implant (CI). The core of the implant is an electrode array that is inserted into the cochlea and electrically stimulates the existing nerve cells there. This is also the main difference to the hearing aid: the hearing aid acoustically amplifies the sound received and relies on the residual function of the hair cells, whereas the cochlear implant directly stimulates the nerve cells electrically.
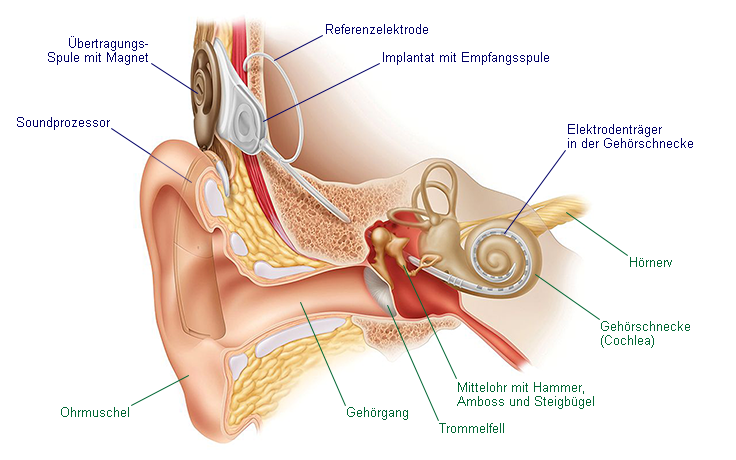
The cochlear implant system consists of two parts: the part implanted during the operation with the electrode array in the cochlea, and the outer part, the sound processor, which is worn behind the ear like a hearing aid. The microphone on the outer part picks up the sound, transmits it to the processor, which converts the sound information into a series of electrical impulses and sends them wirelessly through the skin to the implant via a transmitter coil. The implant stimulates corresponding electrodes in the cochlea, which in turn directly stimulate the existing nerve cells.

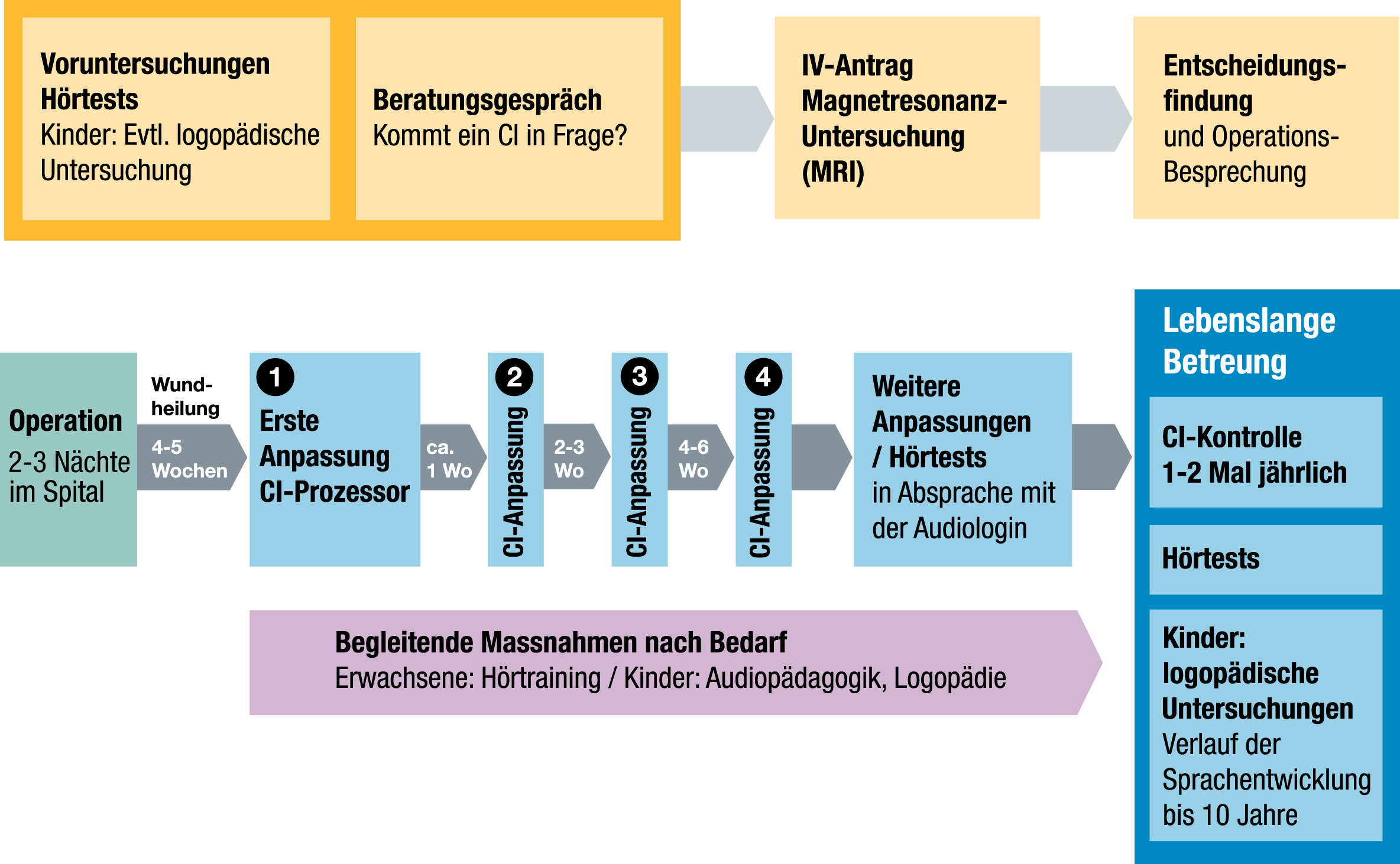
The diagram shows the typical timeline for cochlear implant treatment at the Cochlear Implant Center Zurich. Depending on age, hearing success, etc., deviations are possible.

In children born deaf, the hearing problem is often detected by the newborn hearing test, which usually takes place in the first few weeks of life. Early implantation allows the time of brain maturation and thus speech development to be utilized. Children who are deaf after birth should be assessed as soon as possible with regard to a cochlear implant. If a hearing impairment is suspected, various hearing tests are carried out. If a significant, bilateral sensorineural hearing loss is confirmed, the first step is a trial fitting of hearing aids for a few months and audiopedagogical support. If the parents, the audio educator and the treating physicians do not recognize enough benefit from the hearing aids, discussions are held with all parties involved about a possible cochlear implant fitting. In children, certain examinations are performed under anesthesia. Speech therapy examinations for possible speech development disorders supplement the assessment of children.
 Adults
AdultsIn adults, a series of special hearing tests are carried out to measure hearing loss, assess speech understanding with the hearing aid currently in use and estimate the success of a future cochlear implant. Adults who have been deaf since early childhood are generally not eligible for cochlear implants because their brains cannot process sound.
A magnetic resonance imaging (MRI) of the inner ear and the auditory nerve are the further clarification steps that indicate whether a cochlear implant operation is possible and sensible.
Extensive discussions with the patient and their relatives should highlight the opportunities and limitations of cochlear implant treatment. Once the decision to operate has been made, the IV (disability insurance) or AHV (old-age and survivors’ insurance) and the health insurance company are informed of the planned operation and the costs are applied for.
The first point of contact for parents is the Canton of Zurich’s initial advice center for families with a hearing-impaired child.
To the initial consultation

The operation is performed on children and adults under general anesthesia. After a skin incision behind the auricle, the inner ear is accessed by removing bone from the mastoid process, opened and the implant’s electrode array inserted. The receiver coil is anchored in a recess in the bone. In rare cases, it is necessary to close the external auditory canal and the eustachian tube. The functionality of the implant and the reactions of the auditory nerve are usually checked during the operation. The surgical wound is then closed. The insertion of the electrode array usually results in the loss of residual acoustic hearing.
In the hospital

Medical interventions, examinations or operations on the human body always involve a certain risk of complications, despite compliance with all prescribed safety precautions and medical expertise.
As with any surgical procedure, there is a risk of wound infection despite compliance with all sterility measures. Despite sclerotherapy and closure of all vessels during the operation, post-operative bleeding may also occur in the surgical area. In rare cases, a ringing in the ears (tinnitus) may occur or be intensified or temporary dizziness may be triggered. Due to changes in the inner ear, it is possible that the electrode array cannot be fully inserted into the inner ear or that the tip is folded over during insertion. The surgical approach may result in a taste disorder. As a rule, the surgical wound behind the ear heals quickly. In rare cases, however, wound pain or a loss of sensation and increased scarring may occur.
Late risks include technical implant failure and infection.
Due to today’s surgical techniques and safety measures, facial nerve paralysis is extremely unlikely, as is the risk of cerebrospinal fluid (CSF) flowing from the wound or nose. Due to a progressive infection along the implant, meningitis could occur. An infection, accident or wound healing disorder can lead to implant rejection.
The success of cochlear implantation depends to a large extent on aftercare by competent specialist staff and consistent training in hearing impressions (hearing and speech training). After the initial fitting, repeated checks are carried out in our cochlear implant center to optimize the sound processor.

For children, close cooperation between parents, caregivers, teachers, audiologists and audiopedagogues over many years is a basic requirement. Intensive language training enables the brain to learn to hear and, through language development, to learn to speak. Everyone involved needs time and patience. Children with cochlear implants can achieve spoken language, education and integration in various ways: in schools for the hearing impaired or deaf, but also in mainstream schools with additional therapy and support.

Adults who were able to hear and speak before becoming deaf also need a more or less long adaptation phase before they too can understand speech again. Regular hearing training is therefore highly recommended. This takes place with a recognized audiologist (hearing therapist) near your place of residence. The aim is to provide individual support for hearing development and communication and interaction skills. This includes vowel-consonant exercises, syllable exercises, number and single word comprehension, listening and matching noises and sounds, listening to and understanding factual sentences and texts, telephone training, topic-centered conversations, and the use of technical aids. The hearing training is applied for together with the CI processor at the cost bearer (IV/insurance).
As a patient, you cannot register directly for a consultation. Please get a referral from your primary care physician, specialist. For questions please use our contact form.
University Hospital Zurich
CI Center
ORL clinic
Frauenklinikstrasse 24
8091 Zurich