However, a study by the University Hospital Zurich shows that survival rates for glioblastoma patients in the canton of Zurich have improved in recent years.
The reasons for this are advances in microneurosurgery, even more precise and less stressful radiotherapy, improved treatment with chemotherapeutic agents and new drugs, and treatment by multidisciplinary teams. Many medical disciplines work together in the treatment of brain tumors: Neuropathology, neuroradiology, nuclear medicine, neurosurgery, radio-oncology, neurology and medical oncology.
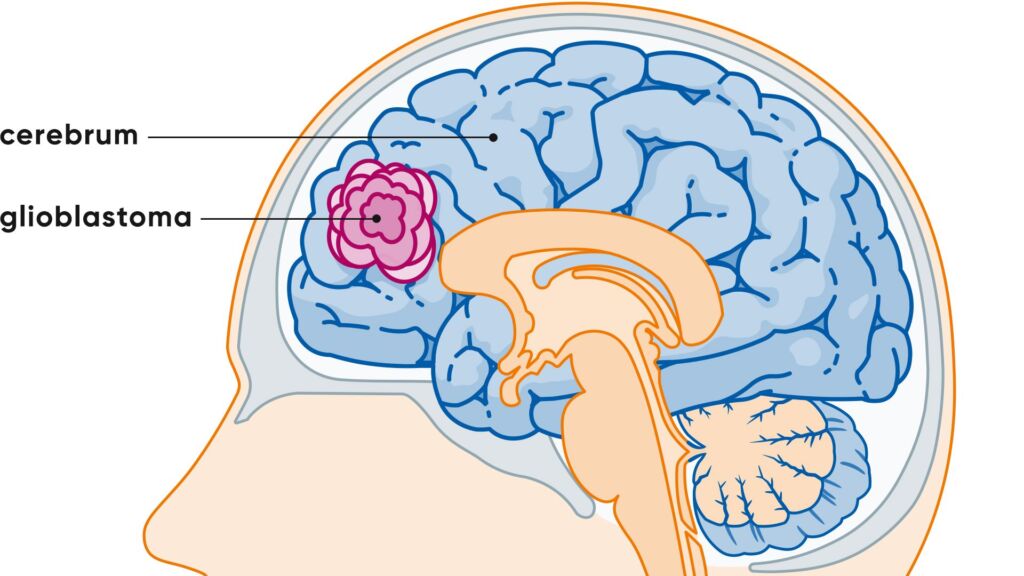
What is a glioblastoma?
Glioblastoma is a malignant brain tumor that develops from so-called glial cells in the brain. It belongs to the group of gliomas and is considered a particularly aggressive growing tumor.
Gliomas presumably develop from the supporting cells of the nerve tissue, the glial cells. Tumors in the brain are classified according to the cell type from which they are thought to originate. In addition, they are classified according to their degree of malignancy. The World Health Organization (WHO) distinguishes between four degrees:
- WHO grade 1: It is a benign tumor that grows slowly and has a favorable prognosis.
- WHO grade 2: The tumor is no longer benign and has a tendency to recur after treatment.
- WHO grade 3: The tumor is malignant
- WHO grade 4: The tumor is very malignant, grows rapidly and has an unfavorable prognosis.
The type diagnosis and the WHO grade are decisive factors for the treatment strategy.
Further terms:
- Astrocytomas: They arise from glial cells and occur in all four WHO grades.
- Glioblastoma: A malignant astrocytoma, WHO grade 4
- Oligodendroglioma: It develops from certain glial cells, the oligodendrocytes, and occurs in WHO grades 2 and 3.
- Ependymomas: They develop from the wall of the ventricles of the brain and occur in WHO grades 1 to 3.
The few known risk factors for the development of glioblastoma include radiotherapy of the brain in childhood and very rare genetic syndromes such as Lynch syndrome or Li-Fraumeni syndrome. Most patients do not have these risk factors.
Frequency and age
In Switzerland, three out of every 100,000 people are diagnosed with glioblastoma every year. Men are more frequently affected than women. The most common age of onset for glioblastoma is between 60 and 70 years of age.
Symptoms: Glioblastoma
Glioblastomas and many other benign and malignant brain tumors can cause many different symptoms and signs. Sometimes they cause headaches, but these can also have completely different (harmless) causes. Many other symptoms may also occur, but these are also not specific to glioblastoma. They can also occur in many other neurological diseases. In particular, the symptoms depend on where in the brain the tumor is located and which centers are affected. Examples are:
- Nausea and vomiting
- Dizziness
- Seizures(epilepsy): Nerve cells “fire” and discharge uncontrollably. Especially in adults, a first seizure is an alarm signal.
- Impaired consciousness – from drowsiness to coma
- cognitive disorders, for example forgetfulness, impaired thinking, concentration and attention
- neurological disorders, for example paralysis, numbness, sensory disturbances (for example for heat, cold, touch, pressure), speech, vision, swallowing, movement and coordination disorders, gait instability
- Changes in personality, for example irritability, aggression, listlessness, apathy, disorientation, anxiety, depression
If the tumor grows and spreads quickly, those affected will feel the first symptoms early on. Seek medical advice if you experience such symptoms.
Glioblastoma – Diagnosis by us
When taking your medical history, it is important that you tell us all the medication you are currently taking. We will ask you about your medical history and ask you to describe the symptoms, their duration and frequency. The diagnosis of glioblastoma involves the following procedure:
A neurological examination by a specialist is the first step in any assessment. This is usually followed by an imaging procedure that provides further clarity. If there really is a brain tumor, then further diagnostics are required to precisely localize it and determine its size and extent. With the help of magnetic resonance imaging (MRI), this is comprehensively possible. Another imaging examination method is positron emission tomography (PET). These examinations are somewhat time-consuming but not painful and are carried out on an outpatient basis.
In order to make a definitive diagnosis, a tissue sample usually needs to be taken. The tumor tissue is obtained during an operation. The surgical procedure also aims to remove as much of the tumor as possible. Sometimes, however, the tumor is in an unfavorable location and surgery is not possible because of the high risk of neurological disorders. In this case, a biopsy is carried out as part of a minor surgical procedure to clarify the diagnosis.
Glioblastoma: prevention, early detection, prognosis
There are no ways to prevent glioblastoma. Screening examinations with MRI, for example, are not carried out because glioblastoma is too rare and because it is not certain that the prognosis would be significantly better if it were detected earlier. The prognosis for this most malignant brain tumor is unfortunately not favorable, but research and medicine have made some progress in recent years and new findings and therapeutic approaches are regularly made.
At the Brain Tumor Center, we will also advise you on whether treatment is possible as part of a clinical trial in order to give you access to new and promising treatment options. We are also happy to provide a second opinion.
Most advanced treatment at the USZ
We will provide you with comprehensive advice if you suspect a glioblastoma or if the diagnosis has already been confirmed. Experts from all disciplines are available to help you with the diagnosis and treatment of your illness. As part of our Brain Tumor Center, we offer a one-stop treatment that aims to meet your personal needs and provide you with the best and most advanced treatment. At the USZ, we have the most modern equipment and therapy procedures at our disposal, enabling us to provide you with an individualized treatment plan. You are also welcome to contact us for a second opinion.
How is a glioblastoma treated?
The treatment of a glioblastoma usually involves several steps and is carried out on an interdisciplinary basis. The aim is to remove as much tumor tissue as possible and to slow tumor growth with further therapies. As standard, the therapy consists of three components:
- Operation: If possible, the tumor is removed microsurgically.
- Radiotherapy: After the operation, the tumor bed is precisely irradiated.
- Systemic therapy: The chemotherapeutic agent temozolomide is administered in parallel with the radiotherapy and subsequently.
This combined form of treatment is now the international standard of care for newly diagnosed glioblastomas.
There is also the possibility of accompanying complementary medical treatment.
New forms of treatment such as Tumor Treating Fields (TTFields) are also available. This non-invasive method uses alternating electrical fields to specifically disrupt the cell division of tumor cells and thus slow tumor growth. The main focus for patients at the USZ is the possibility of inclusion in clinical trials.
How quickly should a glioblastoma be operated on?
A glioblastoma should generally be operated on as soon as possible (within 1-2 weeks) if there is a well-founded suspicion and the patient’s general state of health permits surgery. As this is a fast-growing tumor, it is important to start treatment quickly in order to slow down the progression of the disease and avoid neurological complications.
However, the exact timing depends on several factors, such as the location of the tumor, the severity of the symptoms and the individual risks. The aim of the operation is to safely remove as much tumor tissue as possible without endangering important brain functions.
Frequently asked questions about glioblastoma
The symptoms and signs are very different and depend on which areas of the brain are affected. The first signs often include speech problems, coordination disorders, personality changes or seizures. Many of these complaints develop gradually. It is important to note that even if such symptoms are worrying, they do not automatically indicate a glioblastoma – a neurological examination provides certainty.
In almost all cases, glioblastomas are not inherited. Only in very rare cases – such as certain hereditary tumor syndromes – is there a genetic link. If several people in your family have suffered from brain tumors, genetic counseling may be helpful. As a rule, however, there is no increased risk for family members.
In contrast to many other malignant tumors, glioblastoma practically never forms metastases outside the brain. However, it spreads locally in the brain tissue. It is precisely this local infiltration that makes treatment challenging, as healthy brain functions must be protected.
The life expectancy of a glioblastoma varies from person to person. It depends, among other things, on how well the tumor can be treated and the patient’s general condition. In many cases, the disease is progressive, but there are also patients who remain stable over a longer period of time – especially if various therapies work well. At the USZ, we are also investigating whether innovative forms of treatment can be considered as part of clinical trials. Researchers at the USZ are tracking the world’s largest group of long-term survivors of glioblastoma.
In the last stage of the disease, neurological deficits and physical weakness increase. Orientation or consciousness may also be impaired. In this phase, the focus is on symptom-oriented palliative care: the aim is to alleviate symptoms such as pain or anxiety and maintain quality of life as well as possible. This phase usually lasts from a few weeks to a few months.

