What is tuberculosis?
Tuberculosis (TB for short) is a contagious infectious disease caused by the bacterium Mycobacterium tuberculosis.
Tuberculosis most commonly affects the lungs (pulmonary tuberculosis), but it can affect any organ – such as lymph nodes, bones, kidneys or the central nervous system.
Historically, the disease was also known as “consumption”, “white plague” or “white death”. These terms are considered obsolete today, but some are still known.
Humans are the only relevant pathogen reservoir for Mycobacterium tuberculosis. Transmission occurs almost exclusively through the air, for example when a sick person coughs or speaks. However, not every infection automatically leads to a disease – only 5-10% of those infected develop active tuberculosis in the course of their lives. If treatment is successful, tuberculosis is often cured without leaving any lasting consequences.
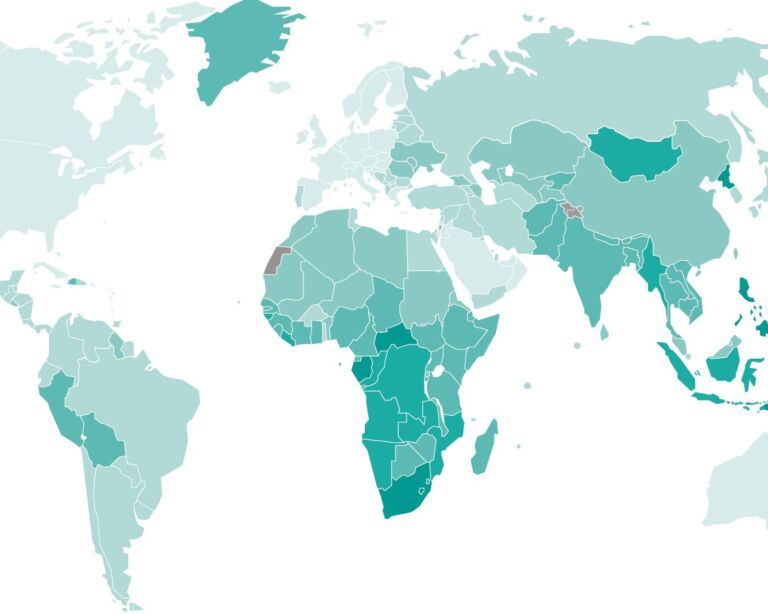
Tuberculosis – frequency and age
There are around ten million new cases of tuberculosis worldwide every year, and around 1.5 million people die from the disease. The countries most affected are in the southern half of Africa and in Asia.
In Switzerland, between 463 and 611 new cases have been reported each year since 2010 (Germany: 4317 to 5915; Austria: 582 to 688). According to the FOPH, most cases of tuberculosis in Switzerland occur in people who come from countries where the disease is still widespread – primarily in Africa and Asia. Half of those affected at home are older people of retirement age who were infected as children. The number of TB deaths in Switzerland is less than ten per year.
In Europe, adults are predominantly affected by tuberculosis, men more than women. In contrast, children often fall ill in countries with a high TB rate. There are many more infected people than sick people. In more than 90 percent of all people infected with TB bacteria, the body’s own immune system is able to keep the pathogens in check or fight them so successfully that no symptoms of the disease appear.
How is tuberculosis transmitted?
The transmission of tuberculosis is aerogenic, via tiny droplets of bronchial secretions. These are released when a person with respiratory tuberculosis coughs or speaks. If inhaled, they can lead to infection in other people.
Transmission of tuberculosis by other routes is much rarer than such an airborne infection. For example, the bacteria can be found in foods such as unpasteurized milk or meat.
Infection with these already rare forms of tuberculosis is extremely unlikely. Transmission can only occur if TB bacteria come into direct contact with another person via a wound or open skin area.
Latent vs. active tuberculosis
Not every infection leads to illness: around 90 percent of all infected people are “latently” infected, i.e. the bacteria are present in the body but do not cause any symptoms and are not contagious. In around 10% of infected people, active tuberculosis develops over time, usually within two years of infection. Symptoms appear during this phase and the disease can be contagious.
Tuberculosis: Causes and risk factors
By far the most common tuberculosis pathogens are rod-shaped bacteria, also known as tubercle bacilli. They come from the mycobacteria family and mostly belong to the species Mycobacterium tuberculosis.
When TB bacteria enter the organism, the immune system tries to fight them with a two-pronged strategy. On the one hand, defense cells encircle the pathogens and form a capsule (a tuberculoma) with them. This is to protect the surrounding tissue. The second strategy: In the center of such a capsule-like cell formation (called a granuloma), specialized scavenger cells (macrophages) take in bacteria in order to destroy them.
If the body’s own defenses succeed in encapsulating the pathogens, calcification and scarring of the tissue can also occur. It can often still be seen on x-rays years later. If the immune system does not succeed in this process, active tuberculosis can develop. If the tuberculosis is connected to the respiratory tract, e.g. pulmonary tuberculosis, it is referred to as “open tuberculosis”; this form of tuberculosis is contagious. The situation is different if other organs are affected rather than the lungs, such as the kidneys, pleura, bones or joints
A weakened immune system in particular is often unable to defeat the bacteria. Another reason why the defense against TB bacteria is not always successful is that they are very robust and can survive passively in the macrophages for a long time. A (latent) tuberculosis that has been kept in check can still break out months or years later.
The higher the number of inhaled bacteria, the greater the risk of a tuberculosis infection. The more of these pathogens are present in a room and the longer a person is exposed to them, the more likely they are to become infected.
People who have been successfully treated for tuberculosis for at least two weeks are generally no longer considered infectious.
What are the symptoms of tuberculosis?
The mycobacteria that cause TB can affect any organ, but in around 70 percent of all cases registered in Switzerland it is the lungs. All forms of tuberculosis usually progress slowly, and the possible symptoms are usually rather mild at the beginning. They include:
- Fever
- General malaise
- night sweats
- Lack of appetite
- Weight loss
In addition, pulmonary tuberculosis often occurs:
- Cough
- Sputum (mucus)
- Chest pain
Important note: If you have bloody sputum or a cough with no known cause, you should urgently consult a doctor.
The possible symptoms of organ tuberculosis:
- Gastrointestinal complaints (with intestinal TB)
- Nodules, thickening and other skin changes (with skin and lymph node TB)
- Shortness of breath (with lymph node TB, the swelling of which constricts the bronchi)
- Nausea, vomiting, stiff neck (in the case of tuberculous meningitis)
How long it takes for the first signs of tuberculosis to appear after infection can vary greatly.
Older patients typically develop fewer symptoms, while children often suffer from prolonged fever or delayed development. There are no clear symptoms that speak exclusively for tuberculosis; the same symptoms could also be seen in neoplastic diseases or autoimmunological diseases, for example. It is therefore initially difficult to make a clear diagnosis of tuberculosis.
As the symptoms of tuberculosis are often only mild at the beginning of the disease and do not differ from those of other diseases (such as influenza), the diagnosis of tuberculosis is difficult to make. First of all, we will ask you about your personal medical history (anamnesis): Since when have you had which symptoms? Is there or was there TB in your immediate vicinity? Any existing risk factors will also be discussed in this first meeting. These include: severe chronic illnesses, a possible HIV infection, the use of immunosuppressive drugs (they weaken the effect of the immune system).
In order to be able to make a reliable diagnosis, the TB pathogens must be detected with a laboratory test.
Tuberculosis: Diagnosis at the USZ
As the symptoms of tuberculosis are often only mild at the beginning of the disease and do not differ from those of other diseases (such as influenza), it is difficult to diagnose tuberculosis. First, we ask about your personal medical history (anamnesis): Since when do which symptoms exist? Is there or was there TB in the immediate vicinity? Any existing risk factors will also be discussed in this first meeting. These include: severe chronic illnesses, a possible HIV infection, the use of immunosuppressive drugs (they weaken the effect of the immune system).
In order to be able to make a reliable diagnosis, the TB pathogens must be detected with a laboratory test.
Tests available for diagnosis:
- A bacteriological analysis under the microscope (usually of coughed up secretions) should determine whether pathogens are present. If so, it is often possible to determine whether the bacteria are TB bacteria by DNA analysis.
- A sample of these pathogens is taken to a laboratory where a bacterial culture is created (the pathogens are cultivated and multiply). Once the desired quantity has been produced, it can be determined whether certain drugs are effective against these pathogens.
- In the tuberculin test, killed TB bacteria are injected under the skin. If a skin reaction (swelling, redness) appears after two to three days, the test is positive. However, it only indicates that the body has had contact with mycobacteria in the past and has now produced defense cells – the tuberculin test is not proof of a current tuberculosis infection.
- The test procedure for adult patients is often an interferongamma test (interferon gamma release assays, IGRA for short). In principle, it works like a tuberculin skin test, but has the advantage that reactions only occur with those mycobacteria that cause tuberculosis (name of the bacterial species: Mycobacterium tuberculosis). However, even this test cannot indicate whether active tuberculosis is present.
- An X-ray examination, often in conjunction with a computer tomography (CT), can make foci of tuberculosis in the lungs visible. X-rays also show the stage of the disease.
Tuberculosis: Prevention, early detection, prognosis
Effective protection against a tuberculosis infection is theoretically only possible by consistently avoiding contact with people suffering from tuberculosis. Of course, this can rarely be checked in everyday life and is impractical.
There is also a vaccination against tuberculosis (BCG vaccination). However, the Swiss vaccination schedule published by the Federal Office of Public Health only recommends this vaccination for newborns and infants younger than 12 months who are at increased risk of infection. These are infants from countries with a high tuberculosis burden. The BCG vaccination is not effective in adults.
Course and prognosis of tuberculosis
The incubation period after infection can last from months to years. Short incubation periods are typical in young children and in people with a weakened immune system. Adults usually experience the symptoms of tuberculosis within two years. In a small proportion of infected people, TB can break out much later. In extreme cases, even after more than a decade.
How the disease progresses depends above all on when it is diagnosed and how it is treated. If the following three conditions are met, there is a good chance that the tuberculosis will heal without leaving any permanent damage:
- The diagnosis is made early.
- The therapy starts early.
- The therapy lasts long enough.
If the immune system of a sick person is weakened (for example after an HIV infection) or if the tuberculosis remains undetected for too long, the course is usually less favorable. Lungs or other organs affected by TB bacteria can then be severely damaged.
Tuberculosis: effective treatment
Tuberculosis is usually treated by administering four different drugs. All four are antibiotics (in this case also called tuberculostatics). Pulmonary tuberculosis (by far the most common form of TB) is usually treated initially with the following active substances:
- Isoniazid
- Rifampicin
- Ethambutol
- Pyrazinamide
When is an operation necessary?
In very rare cases, drug treatment alone is not sufficient. Surgical intervention may then be necessary – for example:
- if parts of the lung are permanently destroyed,
- if larger cavities have formed in the lung tissue (so-called caverns) that do not disappear,
- or if tuberculosis foci in other organs cause complications.
In such cases, a specialized team of doctors decides together whether an operation makes sense.
Treatment of latent tuberculosis
Latent tuberculosis does not cause any symptoms and is not contagious. In order to reduce the risk of subsequent reactivation – especially in immunocompromised persons or persons with risk factors – preventive drug treatment can be carried out. This usually consists of monotherapy with rifampicin over four months or a combination therapy over a shorter period. The aim is to completely eliminate the remaining bacteria in the body.
Frequently asked questions about tuberculosis
Yes, tuberculosis is still widespread worldwide today. Regions in Asia, Africa and Eastern Europe are particularly affected. In Europe and Switzerland, the number of new cases is comparatively low, but the disease has not disappeared. Due to globalization, migration and the increase in antibiotic-resistant pathogens, tuberculosis remains a relevant health issue even in industrialized countries.
A general blood count can give an indication of an inflammatory reaction in the body, but is not sufficient for the diagnosis of tuberculosis. Elevated inflammation values such as C-reactive protein (CRP) or erythrocyte sedimentation rate (ESR) may occur, but do not allow a clear diagnosis. Specific examinations such as microscopic pathogen detection, molecular genetic tests or imaging procedures are necessary for the detection of tuberculosis.
In Switzerland, only active tuberculosis is notifiable. Latent tuberculosis – i.e. the presence of tuberculosis bacteria without clinical symptoms and without risk of infection – is not subject to mandatory reporting. Medical clarification and, if necessary, preventive treatment may nevertheless be indicated, especially if there is an increased risk of reactivation.
Tuberculosis can be cured in most cases with a standardized combination therapy of several antibiotics. Successful treatment requires early diagnosis and consistent drug therapy over a period of several months.
The standard treatment for tuberculosis usually lasts six months. It begins with an intensive phase of two months with four medications, followed by a maintenance phase with two active substances for a further four months. With certain forms of the disease or resistance, treatment can take considerably longer – sometimes up to 12 months or more.
During active and infectious tuberculosis, no activity may be undertaken that could endanger other people. It is usually possible to return to work as soon as there is no longer a risk of infection – usually after several weeks of successful treatment. Whether and when this is the case is decided by the treating specialist on the basis of medical findings.
Tuberculosis used to be referred to by various names, including “consumption”, “white plague” or “white death”. These historical terms refer to the gradual progression of the disease and the high mortality rate before the introduction of effective therapies.