Here at the USZ, you can have the scientifically validated Stockholm3 blood test—which significantly improves the early detection of aggressive prostate cancer—performed. It has been practiced in Sweden and Norway since 2017 and is now also available in other European countries.
Numerous scientific studies involving a total of 75,000 participants have demonstrated the following benefits of the Stockholm3 test:
The Stockholm3 Test
- detects more cases of aggressive prostate cancer,
- reduces the number of unnecessary prostate biopsies (tissue samples taken from the prostate),
- detects aggressive cancer even in men with low PSA (prostate-specific antigen) levels.
Who can take the Stockholm3 test?
The test is suitable for men between the ages of 45 and 75 who have not yet had prostate cancer and whose PSA value is above 1.5 ng/ml.
Stockholm3 at the USZ
If you are interested in a Stockholm3 blood analysis, register now for a consultation.
How much does Stockholm3 cost?
The costs of the Stockholm3 test, all associated consultations relating to the test at our clinic and the PSA test (if necessary) are generally covered by health insurance. The Stockholm3 test is invoiced by the laboratory in Switzerland.
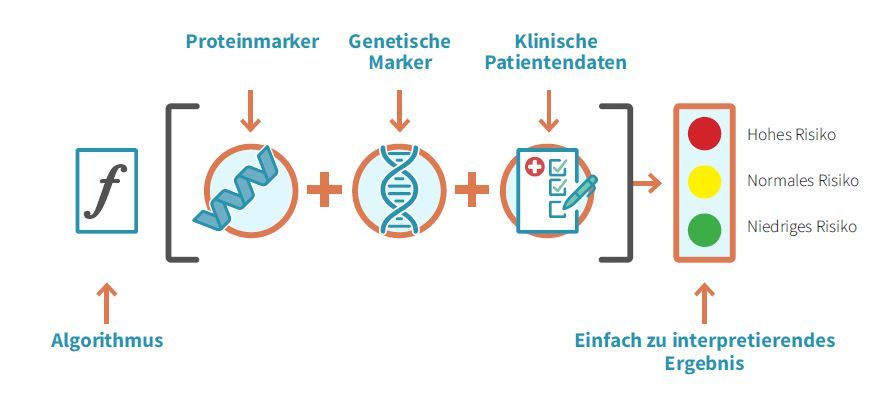
How does Stockholm3 work?
The Stockholm3 test is a blood test. This test can be performed when the PSA level is 1.5 ng/ml or higher. Five different proteins and over 100 genetic biomarkers are analyzed in the blood to determine the genetic risk profile. The current diagnostic standard, PSA (prostate-specific antigen), is also measured during this process. These laboratory test results are combined with clinical data—such as age, previous biopsies, and family history—to calculate a risk score for the early detection of aggressive prostate cancer.
If a patient’s PSA level is 1.5 ng/ml or higher, we can send their blood samples to a Swiss laboratory. After the analysis, the treating urologist receives a clear treatment recommendation. This may mean, for example, that the risk of aggressive prostate cancer is low and that a follow-up screening in 1–6 years is sufficient. Or she may recommend further diagnostic tests, such as an MRI (magnetic resonance imaging) or a prostate biopsy, to determine whether cancer is present. All results are discussed with the patient, and a decision is made on how to proceed.