Gynecology
Operations on the breast
Breast surgery is usually performed under general anesthesia. Special positioning and sterile draping for an optimal surgical result make intubation anesthesia necessary. In the post-operative phase (first hours immediately after the operation), special attention is paid to pain therapy and the prevention and treatment of nausea and vomiting. As with all other gynecological operations, this is done in the recovery room by specially trained nursing staff.
Operations on the female reproductive organs
There are three surgical approaches for operations on the female reproductive organs:
- Vaginal surgery (surgery from the vagina)
- Laparoscopic surgery (keyhole technique)
- Laparotomies (abdominal incision)
Depending on the surgical procedure, different anesthesia methods are therefore possible.
Vaginal operations can be performed under general anesthesia without any problems. However, so-called spinal or epidural anesthesia is also suitable in selected cases. This procedure is comparable to spinal anesthesia for a caesarean section. The patients are awake and can listen to music if they wish or can be given a light sleeping pill if they wish and can then sleep a little during the procedure. For some operations (e.g. insertion of an incontinence band), local anesthesia by the surgeon is combined with simultaneous intravenous administration of a very strong painkiller (= analgosedation). Patients remain awake during the operation but are pain-free.
Many gynecological operations can be performed laparoscopically (so-called minimally invasive). In these cases, general anesthesia is unavoidable because the laparoscopic technique requires the abdomen to be filled with gas and the sleeping patient to be placed in a steep head-down position, which makes artificial respiration necessary.
General anesthesia and spinal anesthesia are usually used in combination for large laparotomies (abdominal operations with a large abdominal incision). An epidural anesthesia is administered before anesthesia is induced, which is continued after the operation and largely guarantees freedom from pain.
Patients are informed about all possible anesthesia techniques and their advantages and disadvantages during the premedication consultation. Qualified specialists with many years of experience are responsible for carrying out the relevant anesthesia services. In the post-operative phase, patients are cared for by competent nursing staff in the recovery room.
Obstetrics
Obstetric pain therapy
In addition to a wide variety of options (massages, acupuncture) for alleviating pain during childbirth, the most common form of pain therapy today is epidural anesthesia (also known as peridural anesthesia). The process has been known for over 100 years and is widely used internationally.
The necessary anesthesiological presence (anesthesiologist and specially trained nursing staff) is ensured around the clock for the building department.
Before the procedure, the anesthetist will discuss with the woman giving birth whether epidural anesthesia is an option or whether there is a situation that speaks against this procedure (a contraindication). At the same time, the possible risks and complications of epidural anesthesia are explained (see below).
We use a combination of spinal and epidural anesthesia (= CSEA) as standard to ease labor and relieve labor pain. In this method, pain conduction, which runs via nerve pathways from the uterus to the spinal cord, is suppressed or strongly attenuated by blocking the pain fibers in the lumbar spine area with medication. The consciousness of the woman giving birth is not impaired.
We usually perform a so-called “walking epidural” with the aim of minimizing or ideally eliminating any weakening of the leg muscles so that the woman giving birth remains mobile. At the same time, it should be possible to push during the actual birth. This is achieved by combining a low-concentration local anesthetic (= local anesthetic) with an opiate supplement. This type of pain relief (analgesia) also has few side effects. Since the beginning of 2020, we have been using an innovative mode, the PIEB scheme. With this method, the local anesthetic is administered intermittently, i.e. with pauses, as a bolus. This has made it possible to reduce the amount of local anesthetic required and at the same time improve the effect of the epidural anesthesia.
Applying pain therapy close to the spinal cord
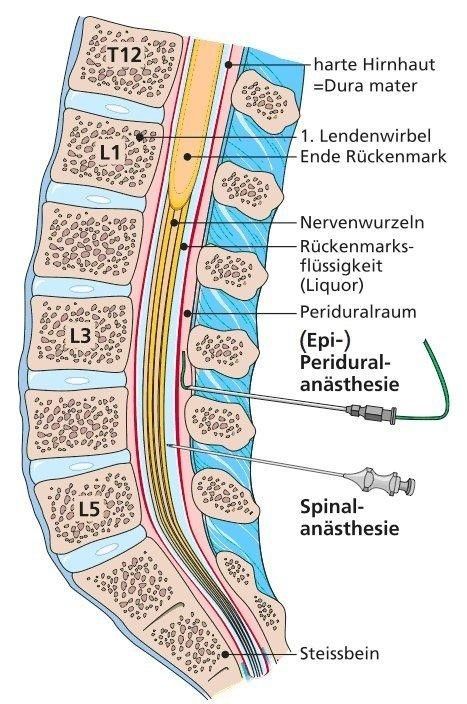
A fine plastic tube (=catheter) is inserted into the so-called epidural space via a hollow needle in the area of the lumbar spine after disinfection and local anesthesia of the skin. After removing the hollow needle, the catheter is fixed to the skin. A pump is then connected, which controls the supply of the painkiller mixture. The device can be operated by the patient herself if required (so-called PCA = patient controlled analgesia) The pain-relieving effect generally takes effect within 10 – 15 minutes. The continuous supply of medication means that the effect can be maintained for as long as necessary.
Should a caesarean section nevertheless become necessary later in the birth, the anaesthetist can increase the effect of the epidural catheter by administering additional local anaesthetics so that it is optimal for the caesarean section.
Possible side effects of spinal pain therapy
Lighter side effects that can be quickly remedied with medication include a drop in blood pressure (possibly combined with nausea) and a slowing of the heart rate. Bladder emptying disorders occur occasionally and may require a single catheterization of the bladder by the midwife. If EDA is performed for many hours, the anesthetic medication may occasionally cause temporary leg weakness.
Serious side effects and complications are extremely rare. For example, although permanent nerve damage (in the sense of impaired sensation or even paralysis) is theoretically possible, it is extremely rare if the blood coagulates well and the procedure is carried out correctly.
Back pain generally occurs relatively often after childbirth, but is neither more frequent nor less frequent after an epidural than without it.
An unpleasant complication, with a frequency of less than 1%, is injury to the hard meninges with the epidural cannula, which can lead to temporary position-dependent headaches when standing and sitting after the birth. These can usually be treated well.
According to current knowledge, epidural anesthesia in the mother is completely harmless for the child.
Caesarean section (caesarean section)
A caesarean section is the most common surgical procedure in obstetrics. In most cases, spinal anesthesia is chosen as the anesthesia method in which a local anesthetic is injected directly into the nerve roots through a very thin cannula in the area of the lumbar spine. This results in a very rapid and intensive anesthesia with complete suppression of pain conduction and temporary elimination of leg motor function (= ability to move).
Advantage of spinal anesthesia: technically relatively simple, very reliable in its effect and safer for the pregnant woman in terms of possible complications than general anesthesia.
If blood coagulation is impaired, in emergency situations or if the expectant mother absolutely refuses regional anesthesia, general anesthesia can be used as an alternative. The patient must be intubated for ventilation during anesthesia and above all to prevent aspiration (gastric juice flowing into the lungs).
