Vascular diseases of the lower extremities
Our aim is to investigate the molecular biological mechanisms that lead to the development of peripheral aneurysms in connection with PAD.
It is usually asymptomatic, with only around 1 – 2% of patients developing critical limb ischemia. These patients are more likely to suffer from coronary heart disease and/or other vascular diseases. Furthermore, stenotic or aneurysmal lesions of the aortic bifurcation are the cause of PAD in more than 95% of all cases [Fowkes 2013].
Our results showed that atherosclerotic lesions and their progression behave similarly in the lower extremities as in carotid arteries [Zimmermann 2015]. As a result, vulnerable plaques can also develop in peripheral vessels, which can lead to a stroke or heart attack.
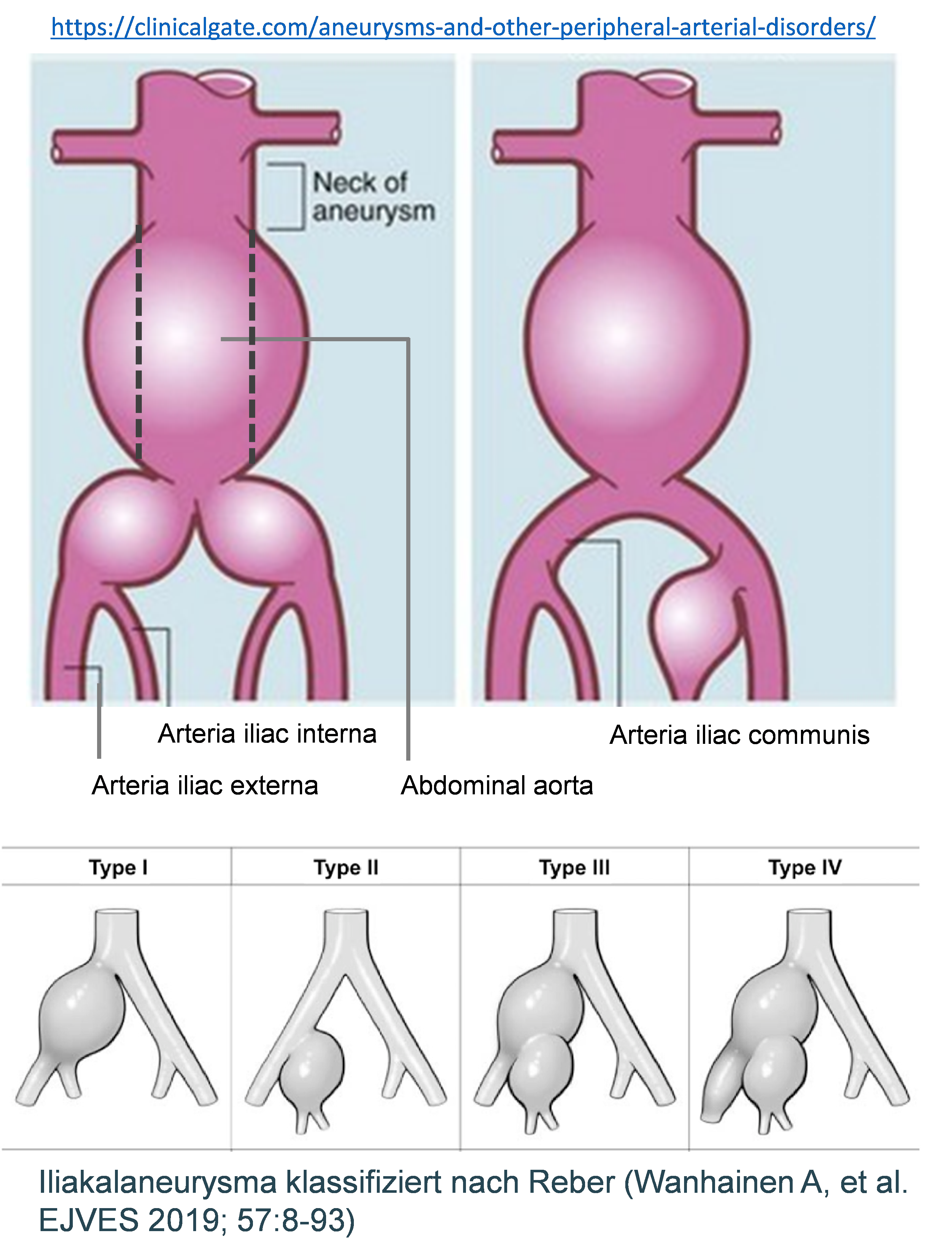
Aneurysm occurs not only in aorta but also in peripheral vessels, especially in male individuals over 70 years of age. In most cases (70%), femoral or iliac arteries are affected (FA, IA). In 25% of cases, peripheral aneurysms are associated with abdominal aortic aneurysms (AAA), which complicates the clinical picture and significantly increases the risk of further complications.
We therefore focus in particular on patients with complex aneurysms including AAA and femoral/iliac aneurysms. Our aim is to elucidate the molecular-biological mechanisms that lead to the development of aneurysms in the lower extremities in connection with pre-existing PAD. Furthermore, we compare the processes and changes in the vessel wall between AAA and FA/IA to determine existing differences.
To do this, we use the latest techniques such as proteomics, transcriptomics and scRNA sequencing. Among other things, smooth muscle cells (SMCs) and endothelial cells (ECs) isolated from the affected patients are analyzed.
- Fowkes FG, et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis. Lancet. 2013;382(9901):1329-40.
- Wildgruber M, Aschenbrenner T, Wendorff H, Czubba M, Glinzer A, Haller B, Schiemann M, Zimmermann A, Berger H, Eckstein HH, Meier R, Wohlgemuth WA, Libby P, Zernecke A. The “Intermediate” CD14++CD16+ monocyte subset increases in severe peripheral artery disease in humans. Sci Rep. 2016;6:39483.
- Rasper M, Wildgruber M, Settles M, Eckstein HH, Zimmermann A, Reeps C, Rummeny EJ, Huber AM. 3D non-contrast-enhanced ECG-gated MR angiography of the lower extremities with dual-source radiofrequency transmission at 3.0T: Intraindividual comparison with contrast-enhanced MR angiography in PAOD patients. Eur Radiol. 2016;26(9):2871-80.
- Zimmermann A, Senner S, Eckstein HH, Pelisek J. Histomorphological evaluation of atherosclerotic lesions in patients with peripheral artery occlusive disease. Adv Med Sci. 2015;60(2):236-9.
- Zimmermann A, Wendorff H, Schuster T, Auer F, Berger H, Eckstein HH. Interobserver agreement of the TASC II classification for supra- and infrainguinal lesions. Eur J Vasc Endovasc Surg. 2010;39:586-90.