What is hyperthyroidism?
A typical feature of hyperthyroidism is that the production and release of hormones in the thyroid gland are abnormally increased. This has serious consequences – the thyroid hormones T3 (triiodothyronine) and T4 (thyroxine) are involved in the control of numerous vital metabolic processes. These include growth and development processes, energy metabolism, heart rate and blood pressure. Fully developed disease associated with symptoms is called manifest hyperthyroidism. In contrast, “hidden” (subclinical) hyperthyroidism is not (yet) noticeable with symptoms – although there are already abnormalities in the hormone status.
Hyperthyroidism – frequency and age
About one in 100 people suffers from hyperthyroidism. In the vast majority of cases, the metabolic disorder is caused by Graves’ disease(Basedow’s disease). This autoimmune disease occurs five to ten times more frequently in women than in men. It usually breaks out between the ages of 20 and 50.
Hyperthyroidism: causes and risk factors
Graves’ disease and so-called thyroid autonomy are the most common causes of hyperthyroidism. More rarely, excess thyroid hormone is due to other causes.
Graves’ disease
In this autoimmune disease, the immune system produces special antibodies – called TRAK (TSH receptor antibodies) – directed against thyroid tissue due to a malfunction. They dock in the thyroid at the same binding sites (receptors) as the thyroid-stimulating hormone TSH. This is secreted by the pituitary gland to control hormone production in the thyroid gland. However, by binding to the receptors of TSH, TRAK mimic its action – boosting the formation of thyroid hormones, detached from brain control.
Thyroid Autonomy
In this case, thyroid tissue escapes regulation by higher-level brain centers (hypothalamus, pituitary gland) and produces thyroid hormones uncontrollably. Experts distinguish three forms of thyroid autonomy:
- Disseminated thyroid autonomy: Autonomous tissue that produces hormones in an uncontrolled manner is found throughout the thyroid gland.
- Unifocal thyroid autonomy: autonomous tissue is confined to a benign “nodule” in the thyroid gland (called an autonomous thyroid adenoma).
- Multifocal thyroid autonomy: there are multiple benign “nodules” in the thyroid gland that produce hormones unregulated by the brain.
Thus, the amount of autonomous tissue in the thyroid gland – and thus the excess of hormones – can vary. Therefore, hyperthyroidism may be more or less pronounced in thyroid autonomy.
Other causes of hyperthyroidism
In rare cases, hyperthyroidism has causes other than Graves’ disease or thyroid autonomy:
- Inflammation of the thyroid gland (thyroiditis)
- Thyroid Cancer
- Excessive iodine intake, for example due to the iodine-containing medication amiodarone (medication against cardiac arrhythmia) or iodine-containing contrast media
- benign tumor of the pituitary gland (pituitary adenoma) that produces excessive amounts of TSH, causing the thyroid gland to overproduce hormones
- Overdose of thyroid hormones, such as those taken to treat hypothyroidism
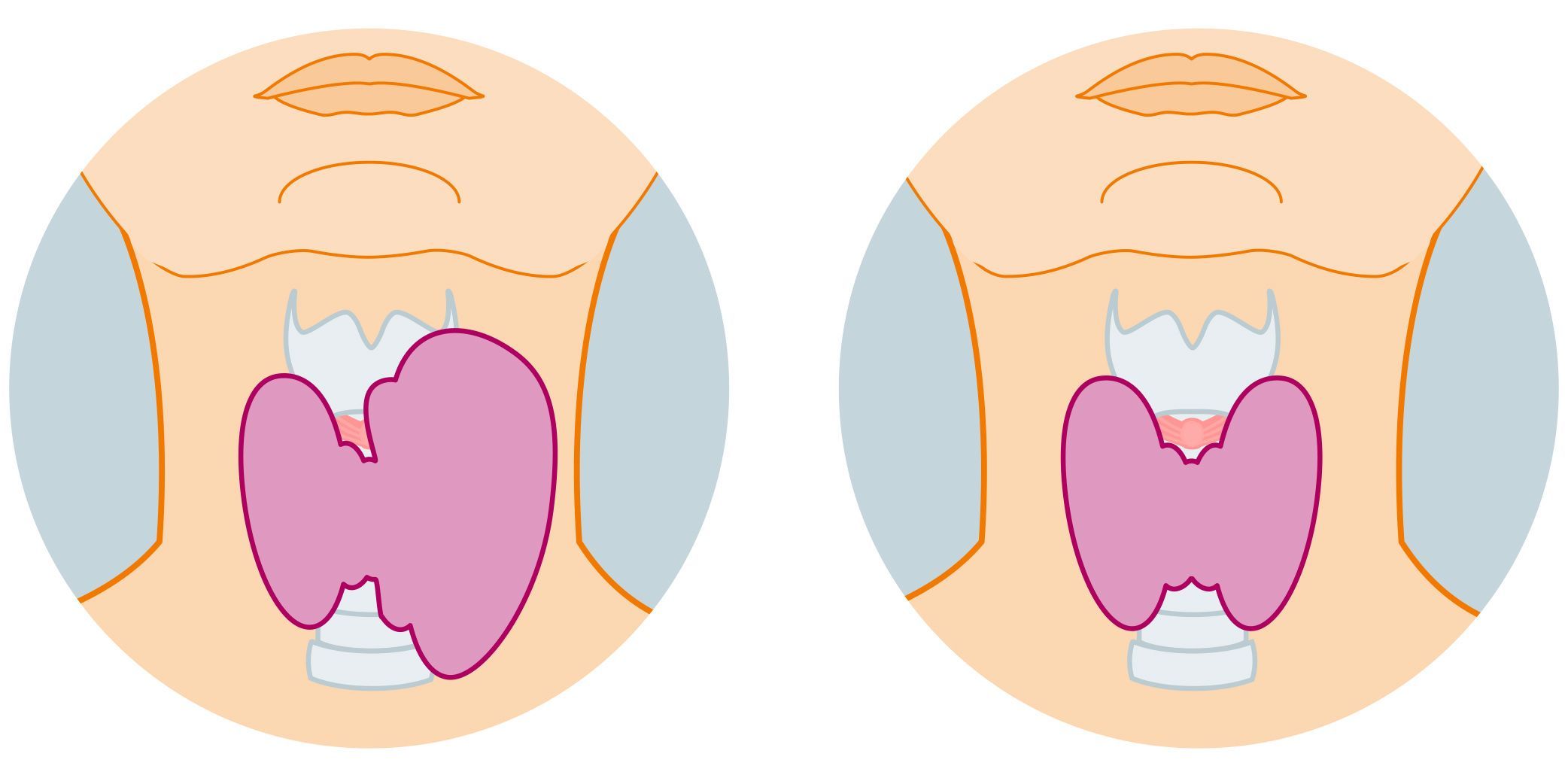
Left: hyperfunctioning thyroid, right: healthy thyroid
Hyperthyroidism symptoms
The hormone excess accelerates metabolic processes in various organs and organ systems. Accordingly, the symptoms of hyperthyroidism can be varied. Possible symptoms include:
- nervousness, restlessness, irritability
- Mood swings
- Trembling
- increased sweating
- warm-moist skin
- Hypersensitivity to heat
- Insomnia
- High blood pressure
- Palpitations, sometimes also cardiac arrhythmia
- Shortness of breath
- Weight loss (despite ravenous appetite)
- Diarrhea
- Hair loss
- Weakness, fatigue, decrease in performance
In addition, hyperthyroid patients often have visibly enlarged thyroid glands, which shows up as swelling in the front of the neck. It is colloquially called goiter. Experts refer to an enlarged thyroid gland as goiter. A typical feature in people with Graves’ disease is protruding eyeballs (colloquially: goggle eyes, medically: exophthalmos). Other eye problems such as photophobia, increased tearing, reddened eyes, or even very dry eyes are also more common in Graves’ disease.
Hyperthyroidism – Diagnosis at the USZ
The first step in the clarification of a possible hyperthyroidism is the medical history: We ask you in detail about your symptoms and any underlying and previous diseases. We will also inquire if you are taking any medications. This will give you a picture of your medical history. The interview is followed by a physical examination. Among other things, we will palpate your thyroid gland to check for enlargement and nodule formation. We also look to see if you have eye problems or even bulging eyeballs, typical of Graves’ disease.
Measurement of hormone levels
Information about your thyroid function can be obtained by measuring hormone levels in your blood. The focus is on blood levels for the thyroid-stimulating hormone TSH and the thyroid hormones T3 and T4 (in free form, i.e. not bound to a protein: fT3 and fT4):
- TSH decreased, fT3 increased, fT4 (mostly) increased: There is a fully developed hyperthyroidism associated with symptoms (manifest hyperthyroidism).
- TSH decreased, fT3 and fT4 normal: There is a “hidden” (subclinical) hyperthyroidism – the thyroid gland still produces normal amounts of hormones despite a decreased TSH value.
If your hormone levels are indicative of hyperthyroidism and you have the symptom trio of goiter, bulging eyeballs and palpitations, you most likely have Graves’ disease. The suspicion is confirmed when TSH receptor antibodies (TRAK) are detected in your blood.
Imaging techniques
- Ultrasound: By means of ultrasound we can examine the position, size, shape and structure of the thyroid gland. This also allows any existing nodes to be assessed more accurately.
- Scintigraphy: The metabolic activity of thyroid nodules can be determined by means of scintigraphy For this purpose, you are first injected with a small amount of a radioactively labeled substance, which accumulates in the thyroid tissue – preferentially in areas with increased hormone production. This different distribution can be visualized by measuring the radiation emitted by the radioactive substance with a special camera. This allows us to distinguish between “hot” and “cold” nodes:
- “hot” nodules: Thyroid nodules with increased hormone production
- “cold” nodules: Thyroid nodules that do not produce hormones or produce only reduced hormones
Hyperthyroidism: prevention, early detection, prognosis
The main causes of hyperthyroidism – Graves’ disease and thyroid autonomy – cannot be prevented in any known way. However, you can do something about other (rarer) causes of hyperthyroidism:
- For a healthy thyroid you should pay attention to an adequate iodine intake: Adults should consume about 180 to 200 micrograms of iodine per day, but never more than 500 micrograms! Excessive iodine intake (also, for example, via iodine-containing medications) can trigger hyperthyroidism.
- Do not take thyroid hormones in overdose if you have been prescribed such medication due to hypothyroidism. Otherwise you will flood your body with too much thyroid hormone, which triggers symptoms of hyperthyroidism.
Hyperthyroidism – course and prognosis
If hyperthyroidism is treated properly, affected individuals can usually lead a normal life.
However, without (adequate) treatment, hyperthyroidism can cause serious health problems. These include cardiovascular problems such as atrial fibrillation (a form of heart rhythm disorder) or heart failure, and osteoporosis (caused by accelerated bone degradation).
A very rare but life-threatening complication of hyperthyroidism is the so-called thyrotoxic crisis. Possible triggers include inadequate hyperthyroidism treatment, excessive iodine intake, infections, surgery, or poorly controlled diabetes mellitus. Signs of thyrotoxic crisis include:
- high fever and sweating
- Vomiting and diarrhea
- Restlessness and anxiety
- Cardiac arrhythmias
- Impaired consciousness up to coma and circulatory failure
Anyone who develops a thyrotoxic crisis must receive intensive medical treatment as quickly as possible – there is a danger to life!
Thyroid Consultation
The thyroid consultation at the Clinic for Endocrinology, Diabetology and Clinical Nutrition or the thyroid consultation at the Clinic for Nuclear Medicine treats patients with thyroid or parathyroid disorders.
Hyperthyroidism: Treatment planned individually
There are three options for hyperthyroidism treatment:
- Medication
- Radioiodine therapy
- Surgery
Which of these therapies is most appropriate depends on several factors. These include the severity of the disease, the size and structure of the thyroid gland, the age and the general health of the affected person. Possible pregnancy or breastfeeding also influences the choice of therapy (no radioiodine therapy). Last but not least, the cause of hyperthyroidism also plays an important role.
Frequently asked questions about hyperthyroidism
Hyperthyroidism often makes you feel nervous, irritable and restless. Symptoms such as palpitations, sleep disorders, increased sweating and weight loss may occur.
An untreated hyperthyroidism can be dangerous as it puts a strain on the cardiovascular system and can lead to cardiac arrhythmia or osteoporosis. In rare cases, a life-threatening thyrotoxic crisis may occur.
If you have hyperthyroidism, you should avoid excessive iodine consumption, for example through iodine-containing medication or food supplements. Stress and physical overexertion can also exacerbate the symptoms.
Hyperthyroidism is often easily treatable, but the treatment depends on the cause. In many cases, it can be controlled or eliminated by medication, radioiodine therapy or surgery.
