In SLE, every organ system can potentially be affected. SLE is characterized by the formation of numerous autoantibodies. The partially scarred, reddened skin lesions that occur when the skin is affected gave the disease its name (lupus is Latin for wolf), as they appear to devour the flesh “as a wolf would”.
Overview: What is lupus?
People with SLE describe very different symptoms. The most common symptoms are pronounced tiredness (fatigue), migrating joint pain (oligoarthralgia), dryness of the mucous membranes (sicca symptoms), hair loss and recurring mouth ulcers. The typical “butterfly exanthema” on the face occurs in around a third of patients. It is a raised, symmetrical reddening of both cheeks with a connection over the bridge of the nose and on the forehead. In more than 50 percent of those affected, the kidneys are affected.
The disease can be intermittent or (more rarely) permanently active. The aim of treatment is to keep the activity of the disease as low as possible and to use small amounts of glucocorticosteroids (GCS). It is particularly important to recognize the kidney infestation and other vital organs quickly, as early and correct treatment prevents complications. The manifestation of the disease in terms of organ manifestations and severity is very individual, which makes the therapy very different. Some symptoms such as fatigue (tiredness) and sicca symptoms (dryness of mucous membranes) are difficult to treat. SLE, with its diverse manifestations and occurrence of autoantibodies, is the prototype of an autoimmune disease and belongs to the group of inflammatory connective tissue diseases (collagenoses).
Systemic lupus erythematosus: Frequency and age
SLE mainly affects women of reproductive age (20 – 30 years). Men are affected in only one in ten cases. In Switzerland, it is estimated that around 1,200-4,000 patients are affected by SLE. Experts estimate that 20 to 50 people per 100,000 are affected.
Lupus disease: causes and risk factors
In most cases, the development of SLE is multifactorial. The following factors can contribute to this:
- Genetic/polygenetic factors (Although SLE is not a hereditary disease)
- Infections (viral infections can trigger an autoimmune disease such as SLE)
- Female hormones probably play a role
- Certain medications can trigger SLE
- Nicotine consumption
Lupus symptoms: SLE begins with fatigue and fever
Systemic Lupus Erythematosus can lead to very different symptoms. In addition to tiredness and feeling ill (“like the flu“), those affected may suffer from the following symptoms:
- Fever
- Sensitivity to sunlight
- Weight loss and loss of appetite
- Hair loss
- Mucosal changes in the mouth (aphthae)
- White coloration of the fingers in cold weather (Raynaud’s syndrome)
- Joint pain and swelling
Butterfly erythema occurs in around 30 percent of cases: red, raised skin lesions on both cheeks, the forehead and the bridge of the nose. If left untreated, this can leave deep scars. Many sufferers seek medical advice due to swollen and painful joints. If the disease is not recognized in time, other organ systems can be affected. The pleura, pericardium or heart valves can become inflamed. Blood count changes are very common. Kidney inflammation (lupus nephritis), which can lead to kidney failure and dialysis, is a serious threat.
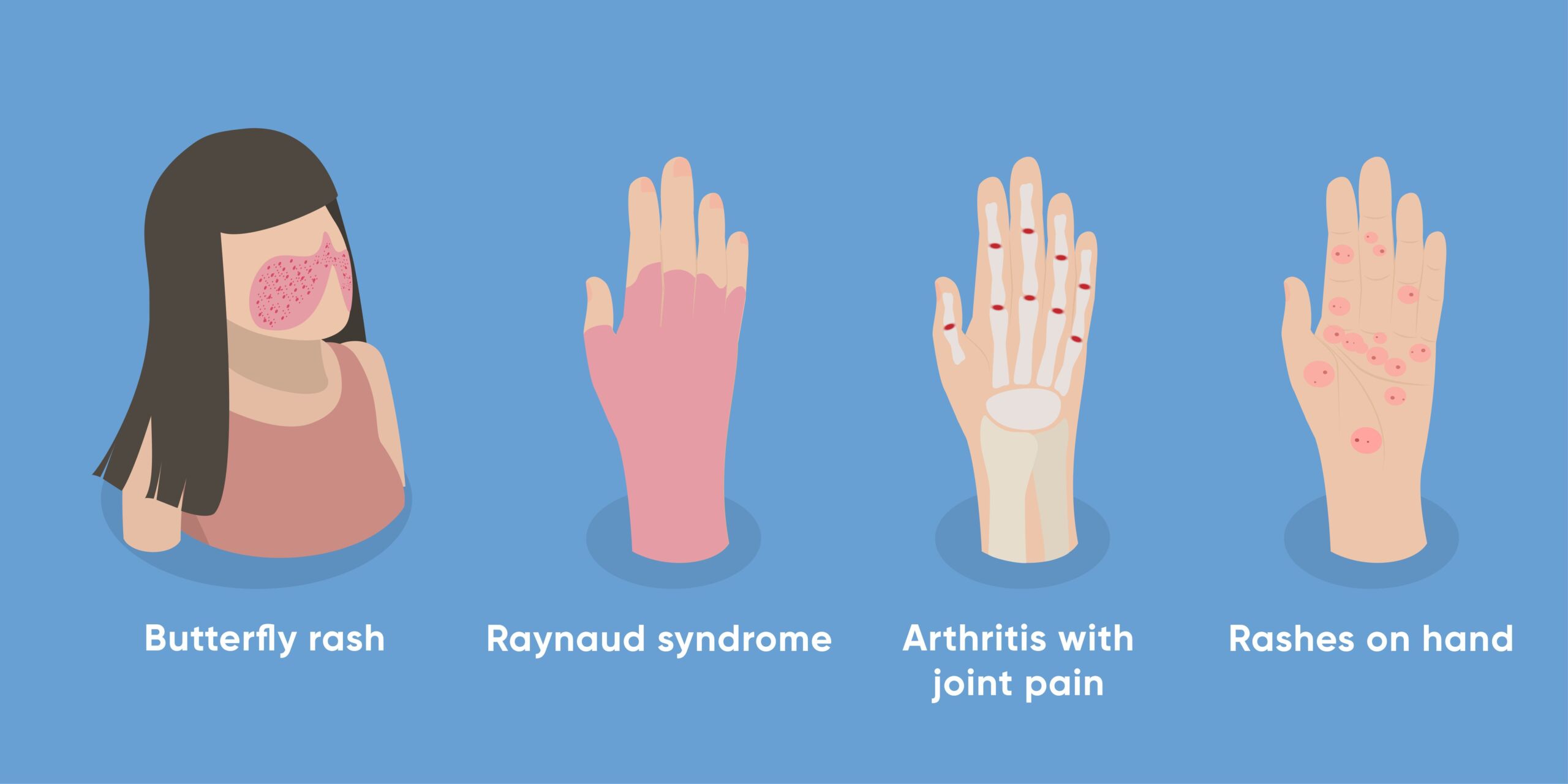
Possible symptoms of lupus
How the body reacts to SLE
In SLE, the normal processes of “apoptosis” (cell disposal) are disturbed. This brings components of the cell nuclei into contact with the immune system. This process leads to an activation of the immune system. As part of this immune activation, antibodies are produced which are directed against the body’s own cell nuclei (anti-nuclear antibodies = ANA). Since cell nuclei are present in all organs, this immune reaction can take place in practically any organ. The disease usually progresses in relapses at irregular intervals.
Diagnosis of SLE disease at the USZ
In the absence of a typical butterfly exanthema, the diagnosis of SLE can be very difficult. We first take a detailed medical history and document all symptoms. This is followed by an examination of the skin, lymph nodes and joints as well as an examination of the internal organs. Laboratory tests are always part of the clarification. We are looking for the typical autoantibodies that occur predominantly in SLE. The measured values in the blood may show the following deviations:
- Increased erythrocyte sedimentation rate
- Consumption of complement factors C3 and C4
- Reduced number of white and red blood cells and platelets
- Occurrence of autoantibodies (ANA) with the lupus-specific anti-dsDNA antibodies and anti-Smith antibodies
A urine test is also routinely carried out. If the kidney is affected by SLE, red blood cells, white blood cells and/or increased protein excretion are typically detectable. Kidney involvement is accompanied by no pain and is hardly noticed by patients. Indications may be increased blood pressure, edema or foamy urine. If symptoms are present, it may be necessary to take a skin sample or kidney tissue in order to make a diagnosis.
Detecting lupus: experience makes the difference
You will therefore receive the best possible treatment at a specialized center such as the USZ. At the USZ, we have the knowledge and experience to recognize the disease even in difficult cases. We always endeavor to treat the disease in accordance with the latest scientific findings. USZ clinics are also taking part in worldwide studies to develop new therapies for SLE.
In order to provide optimal care for patients with SLE and kidney disease, the Clinic for Kidney Diseases (Nephrology) at the USZ has its own special consultation hours. Furthermore, an interdisciplinary consultation hour was established at the Immunology and Nephrology Clinics for SLE patients. In addition, regular boards are held to discuss difficult courses of disease on an interdisciplinary basis and to find optimal treatment solutions.
Criteria that indicate SLE
New classification criteria were established in 2019 to better recognize the disease. This was the first time that the American (ACR = American College of Rheumatology) and the European (EULAR = European League against Rheumatism) rheumatic disease associations had worked together. Patients with ANA can be classified if the antibodies and/or symptoms cannot be explained by another disease. The following symptoms or organ systems are considered in the classification with regard to the diagnosis of SLE:
- Constitutional: Fever
- Skin: non-scarring alopecia or oral ulcers or subacute cutaneous or discoid lupus or acute cutaneous lupus (butterfly)
- Joint involvement: synovitis in at least two joints or tenderness in at least two joints and morning stiffness for at least 30 minutes.
- Neurology/psychiatry: delirium or psychosis or epilepsy
- Serositis: pleural or pericardial effusion or acute pericarditis
- Hematology: leukopenia, thrombocytopenia or autoimmune hemolysis
- Kidney: proteinuria > 0.5g/24h; class II or V LN; class III or IV LN
- Immunological domains
- Antiphospholipid antibodies: Anticardiolipid AK IgG >40 GPL or Anti-Beta2GP1 IgG > 40 U or Lupus anticoagualns
- Complement proteins: C3 and/or C4 consumption
- SLE-specific antibodies: anti-dsDNA AK or anti-Sm AK
Lupus prevention, early detection and prognosis
If you notice symptoms such as noticeable reddening of the skin, sensitivity to the sun, swollen joints, increased tiredness (fatigue) or recurring fever, you should seek medical advice. It is important to avoid sun exposure and tobacco consumption. Thanks to new drugs, improved diagnostic options and a better understanding of the disease, life expectancy and quality of life for those affected have improved significantly in recent years. Today, people with SLE have an almost normal life expectancy. However, sufferers often have to take long-term medication. Damage to the kidneys and other internal organs is a particular risk, as are the long-term effects of cortisone therapy.
Self-help groups
The exchange with people who are affected by the same disease can be a great support in coping with the disease. Advice on finding a suitable self-help group is available from
Selbsthilfe Zürich. Self-Help Zurich and the University Hospital Zurich are cooperation partners in the national project “Health literacy thanks to self-help-friendly hospitals”.
Special consultation: Systemic lupus erythematosus (SLE)
The special consultation “Systemic lupus erythematosus (SLE)” is aimed at patients with a systemic manifestation of SLE.
Lupus treatment
SLE cannot be cured. The aim of the therapy is to prevent organ damage and alleviate symptoms. As long as a sick person has hardly any symptoms, they do not need to take any other medication apart from antimalarials (hydroxychloroquine). However, regular medical check-ups and examinations when new symptoms occur are important. The aim is to recognize changes quickly and initiate countermeasures in good time before organs are damaged. Psychological support is also important for many sufferers in order to come to terms with this difficult to categorize illness. The treatment depends on the symptoms and findings of the patient. In particular, sun exposure prophylaxis, antimalarials, anti-inflammatory agents (cortisone) and immunosuppressants (to suppress the body’s own immune system) are used.
Details of the treatments
Frequently asked questions about lupus
It is important to have regular medical check-ups, avoid exposure to the sun, tobacco consumption and stress, and to adhere to drug therapy.
In principle, there are no restrictive diets. However, for a generally healthy lifestyle, foods that promote inflammation such as highly processed products (ready meals, meat products, etc.), a diet rich in trans fats and carbohydrates and excessive salt consumption should generally be avoided.
Abnormal blood values include the detection of anti-nuclear antibodies (ANA) and specific autoantibodies against dsDNA, SmD, chromatin, ribosomal P protein or C1q, occasionally reduced complement activities of the classical pathway with reduced complement factors C3 or C4, as well as changes in white and red blood cells.
UV radiation, stress, infections and tobacco consumption can exacerbate symptoms and disease activity.
Lupus can cause inflammation of the lacrimal glands, eye muscles, retina or vascular changes and lead to eye dryness, pain and swelling, and in rare cases to visual disturbances or blindness.