The laboratory of the Department of Immunology offers a wide range of serological diagnostics for hepatitis. In the context of hepatitis B and E infections, we also offer molecular diagnostics to detect the viral load or determine the genotype and possible mutations.
Laboratory diagnosis of hepatitis A
The laboratory of the Department of Immunology offers serological diagnostics for hepatitis A. IgG and IgM antibodies are detectable as soon as the patient shows symptoms. After an infection, only the IgG type antibodies are still present. The same picture emerges after a vaccination. Infection and vaccination cannot be distinguished.
Phase
Anti-HAV IgG
Anti-HAV IgM
Late incubation phase
–
–
Acute infection
+
+
Expired infection/vaccination
+
–
Polyclonal stimulation in the context of another infection
+
–
Laboratory diagnostics for hepatitis B and D
Hepatitis B
The diagnostic laboratory of the Department of Immunology offers comprehensive diagnostics for hepatitis B. The serological patterns can be used to differentiate between acute and chronic infections or infections that have already occurred, as well as to detect a vaccination.
Course of acute hepatitis B. Source [1]
Course of chronic hepatitis B infection.
Anti-HBc antibodies are markers for contact with the hepatitis B virus. While the HBs antigen signals the current presence of the virus, the detection of anti-HBs antibodies means that the infection has been overcome. After vaccination, only anti-HB antibodies are detectable, as only the surface antigen is immunized.
Phase
HBs antigen
Anti-HBc IgM
Anti-HBc IgG/IgM
Anti-HBs
Anti-HDV
Acute infection
+
+
-/+
–
Chronic infection
+
–
+
–
Status after hepatitis B
–
–
+
+
–
Status after vaccination
–
–
–
+
–
Hepatitis D infection
+
+/-
+
–
+
Further parameters are available for more specialized questions. The HBe antigen (secreted by-product of the HBc antigen, which dampens the immune reaction against the HBc antigen) is an indication of active virus replication with high viremia. In an earlier old model, hepatitis B infection was divided into two phases, with the replicative phase associated with high HBe antigen, high HBs antigen, high viremia and marked inflammatory response (histology) and highly elevated transaminases.
Phases of hepatitis B infection (old model)
Phases of hepatitis B infection (new model)
The replicative phase was followed by a non-replicative phase, characterized by the seroconversion of the HBe antigen to anti-HBe. This phase characterized the patient as a healthy carrier. In the meantime, this two-phase model has been replaced by a four-phase model. A distinction is made between a phase of immune tolerance (high viremia, detection of HBe and HBs antigen without inflammatory activity and normal transaminases), a subsequent immunoreactive phase with a strong inflammatory reaction, a third, low-replicative phase (HBs antigen persistence, seroconversion to anti-HBe, significant reduction in viral load and normal transaminases) and finally a possible reactivation phase (characterized by HBs antigen persistence, fluctuating elevated transaminases and viremia with negative HBe antigen). In the new model, HBe antigen-negative chronic hepatitis is therefore regarded as reactivation after inactive carrier status, whereas in the old model it was regarded as a transition to healthy carrier. In addition, there are mutations that cannot form an HBe antigen and still have high viral loads. Today, virus replication is quantified by direct detection (PCR) of HBV DNA. The distinction between HBe antigen-positive and HBe antigen-negative chronic hepatitis is nevertheless useful because the course and response to treatment is different in the two groups [3].
As the immunological screening tests are highly sensitive, false reactive results may occur. If the HBs antigen is detected, HBs antigen confirmation is carried out. An HBs antigen-neutralizing antibody is added and then measured again.
There are cases in which only HBc antibodies can be detected, but no HBs antigen or anti-HBs antibodies. The so-called “anti-HBc only” findings can have the following possible explanations: The anti-HBs antibodies have fallen below the detection limit, as the infection occurred a very long time ago, or it is an HBs antigen-negative infection (HBs antigen mutants), testing in the “window phase” (no more HBs antigen and still no anti-HBs antibodies) of a fading infection is also theoretically possible. Direct detection by PCR is useful for clarifying infectivity. PCR is also used for therapy monitoring.
HBV genotyping and resistance testing for the most important mutants of the hepatitis B virus are also offered for the clarification of patients before or during antiviral therapy.
Hepatitis D
The hepatitis D virus is an incomplete RNA virus that requires the hepatitis B virus to replicate. The diagnosis of a hepatitis D infection first requires the detection of a hepatitis B infection. Hepatitis D infection is detected by determining anti-HDV antibodies and by PCR diagnostics.
False reactive values can occur with highly sensitive immunological tests. If the detection of the HBs antigen is questionable, an attempt is made to reverse the result by prior neutralization with an antibody against HBs. If this is successful, it is indeed HBs antigen, otherwise the result must be classified as a false positive.
Analysis
Meaning
HBV DNA, HBV PCR, viral load
Clarification of infectivity, monitoring during therapy
HBV genotype
Response to interferon therapy depends on the genotype
HBV-Drug Resistance
Detection of mutations against important antiviral drugs
[1]: Lothar Thomas – Laboratory and diagnosis
[2]: Müller Ch. Chronic HBeAg-negative hepatitis B-a confusion. Journal for Gastroenterological and Hepatological Diseases 2008; 6 (2), 10-14
[3]: Prof. Dr. med. Markus Heim, Department of Gastroenterology and Hepatology, University Hospital Basel; Abklaerung und Behandlung der Hepatitis B. tellmed/Fachliteratur/Medizin_Spektrum/MS31, 2006
PCR diagnostics of hepatitis B infection
PCR is available for the direct detection of infectious virus particles (viral load). This determination is important for the assessment of infectivity, e.g. for the isolated detection of anti-HBc and for monitoring before and during antiviral therapy. As the HBs antigen test primarily detects particles that do not contain any DNA, the results of the HBs antigen test cannot be directly compared with the viral load.
For the clarification of patients before or during antiviral therapy, we also offer the determination of HBV genotypes and a resistance test for the most important mutants of the hepatitis B virus.
Analysis
Description of the
Meaning
HBs antigen confirmation
Confirmatory test for HBs antigen
Important for questions about false positive HBs antigen detection
PCR diagnostics of hepatitis D infection
Determination of the HDV viral load is particularly indicated in HBV carriers who show high HBs in serum but have negative or borderline HBV viral loads. The HDV PCR is significantly more sensitive than the determination of the HDV antigen, as the HDV antigen is quickly masked when the anti-HDV antibodies are formed.
Laboratory diagnosis of hepatitis C
As a screening test, antibodies against the hepatitis C virus are determined using an immunoassay. As screening tests must be very sensitive in order to detect all patients with this disease, non-specific reactions can occur. Therefore, a positive result must be further clarified with additional tests. The HCV confirmation test (LIA), which detects antibodies against various antigens of the hepatitis C virus, can be used to confirm the result of the screening test.
As the antibodies against the hepatitis C virus remain detectable for decades, even after the infection has been cured, these two tests say nothing about whether the infection is still active. The detection of HCV RNA using PCR is available for this purpose. A positive PCR result proves an active infection, but a negative test does not completely rule out such an infection (in the case of chronic infection, positive HCV RNA results are occasionally only transient).
Prior to antiviral therapy, the HCV RNA, the so-called viral load, and the HCV genotype are determined. It is also important to determine the viral load if a recent infection is suspected, as the antibodies against the hepatitis C virus only become detectable after six to eight weeks.
Some HCV infections result in cryoglobulinemia . Cryoglobulins are immunoglobulins that precipitate below 37°C and completely dissolve again when reheated to 37°C. According to Brouet, they are divided into three types, depending on whether monoclonal and/or polyclonal immunoglobulin is present. As there are fluid transitions, classification can sometimes be difficult. The HCV infection is type II. Preanalytics is essential in the search for cryoglobulins. If coagulation takes place below 37°C, the cryoglobulins precipitate, remain in the coagulum and can no longer be detected in the supernatant, or only in reduced quantities.
To detect a hepatitis E infection, tests are used to detect IgG and IgM antibodies against the hepatitis E virus.
If both IgG and IgM antibodies are present, it is an acute infection, provided that polyclonal stimulation by another infection, e.g. an EBV infection, is excluded. If IgG antibodies alone are detected, the patient has previously had a hepatitis E infection. If only IgM antibodies are positive, then there is probably an unspecific reaction in the context of another infection.
Phase
Anti-HEV IgM
Anti-HEV IgG
Acute infection
+
+
Status after hepatitis E
–
+
Polyclonal stimulation in the context of another infection
+
–
In addition to this serology, we now also carry out quantitative hepatitis E-PCR . If IgM-AK is detected in the serology, it can be quickly determined whether the infection is actually active. Thanks to the quantitative determination, it is also possible to determine whether the infection is acute or chronic.
Order card for referrers
You can use the order card to order individual analyses. To ensure that your order can be processed properly, it is essential that the order form is completed correctly.
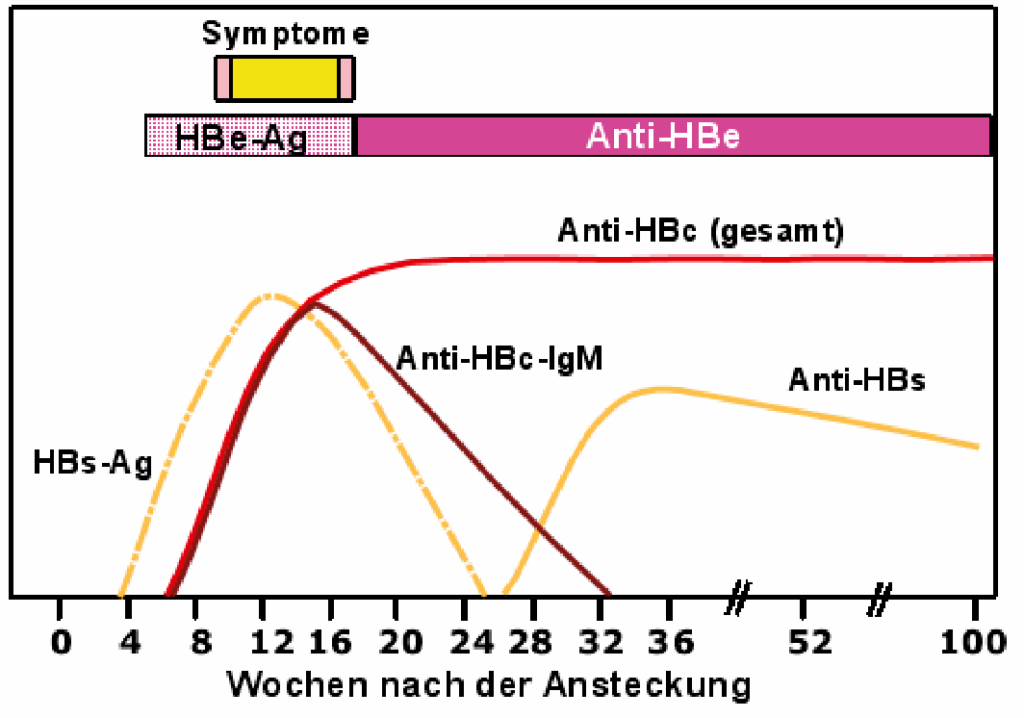 Course of acute hepatitis B. Source [1]
Course of acute hepatitis B. Source [1]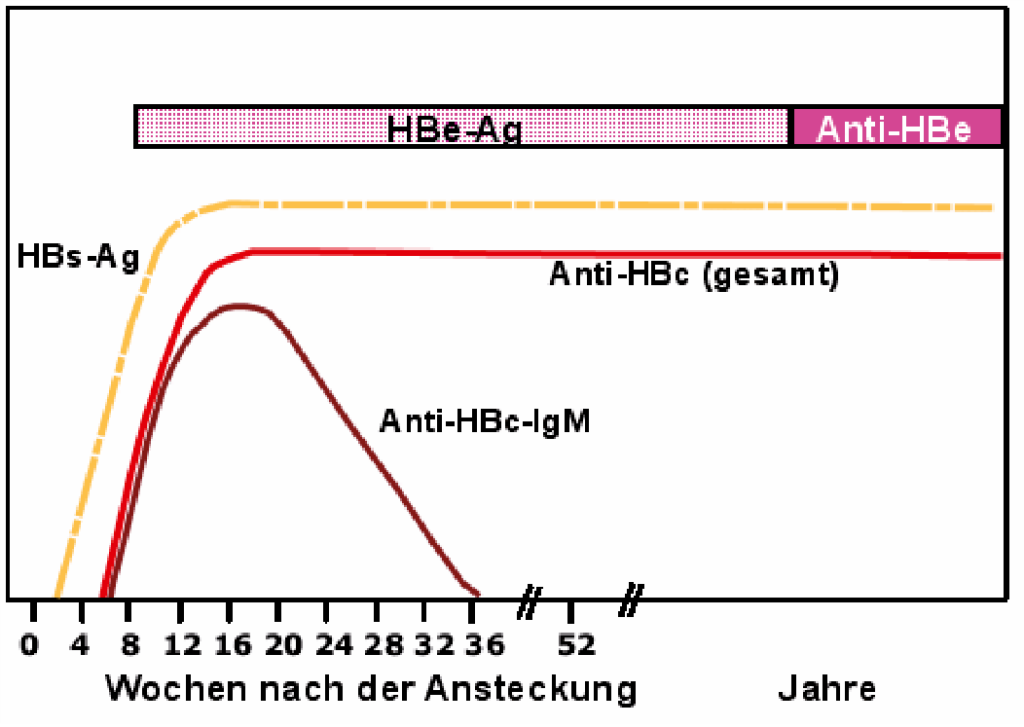 Course of chronic hepatitis B infection.
Course of chronic hepatitis B infection.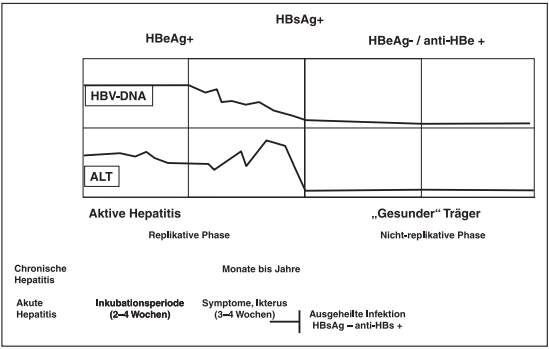 Phases of hepatitis B infection (old model)
Phases of hepatitis B infection (old model)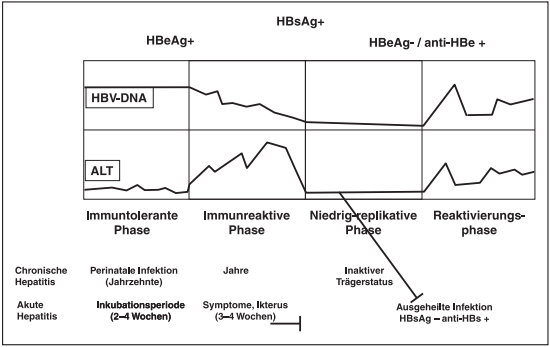 Phases of hepatitis B infection (new model)
Phases of hepatitis B infection (new model)