The Lung Transplant Centre at the University Hospital Zurich is one of the most modern clinics in Switzerland specializing in lungs. Today, bilateral lung transplantation is performed for most surgical indications. It has replaced the heart-lung transplantation used in the pioneering days of lung transplantation. As of December 2019, 547 lung transplants had been performed in Zurich.
Today, lung transplantation is an established therapy for patients with advanced lung diseases, in particular patients with cystic fibrosis, pulmonary fibrosis, chronic obstructive pulmonary disease and alpha-1-antitrypsin deficiency pulmonary arterial hypertension as well as other incurable or rare lung diseases such as lymphangioleiomyomatosis, histiocytosis X and sarcoidosis. Lung transplantation as a form of surgical therapy increases the chances of survival and leads to a significantly improved quality of life.
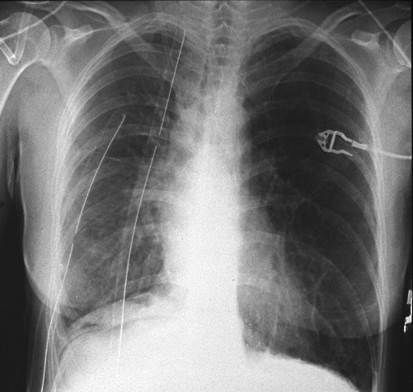
The first successful one-lung transplant (the patient survived for seven years) was performed in Toronto, Canada, in 1983. The first double lung transplant was performed in 1985 (the patient survived for 16 years). In Switzerland, the first patient underwent a lung transplant in Zurich in November 1992 (Fig. 1-3). Switzerland has two lung transplant centers, in Zurich and Geneva, whereby the surgical part of the therapy has been transferred from Geneva to Lausanne since 2004.
Vor der Lungentransplantation.
Nach der Transplantation.
Today, cadaveric donation is still the rule for lung transplants. Due to the increasing shortage of organs, living donation was developed and introduced. However, it is limited to very few experienced centers (in Japan, the USA).
Who will be transplanted?
Lung transplantation is indicated in advanced stages of lung disease and when conservative treatment options have been exhausted. In this phase, patients suffer from dyspnea (shortness of breath) at the slightest exertion, their quality of life is significantly reduced and their estimated life expectancy is just under two years.
Lung transplantation is not indicated for patients with concomitant systemic diseases, malignancy or sepsis (blood poisoning), generalized arteriosclerosis, renal and hepatic insufficiency or with unfavourable psychosocial factors, nicotine, alcohol or drug addiction, or if they are over 65 years of age (according to international guidelines).
Forms of illness
Cystic fibrosis
Cystic fibrosis is a systemic disease that affects various organ systems, including the upper and lower airways, liver, pancreas and gastrointestinal tract. Patients are often colonized with multi-resistant germs at the time of the necessary lung transplant.
Thanks to advances in extremely precise peri- and post-operative care, cystic fibrosis is one of the diseases with the best post-transplant results in experienced centers. Patients should be referred to a transplant center at an early stage, especially before they have lost a significant and usually irreversible amount of body weight due to their progressive underlying disease, leaving them weakened and without muscle strength.
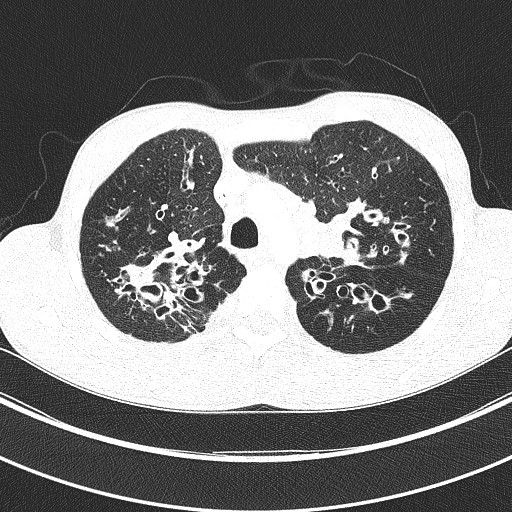
CT thorax: Detectable bronchiectasis in cystic fibrosis
COPD is one of the most common indications for lung transplantation worldwide. On the one hand, this disease is very common; on the other hand, COPD patients on the transplant waiting list have a favorable prognosis compared to patients with other underlying diseases. In principle, unilateral or bilateral transplantation is an option for these patients. Although the operation time is shorter with single lung transplantation, the remaining residual lung poses a risk of complications later on. The functional results and long-term survival are better after bilateral transplantation, which is why we prefer the bilateral variant in Zurich.
Pulmonary fibrosis often leads to a rapid decline in lung function shortly after diagnosis, and in many cases the affected person comes too late for a preliminary assessment for a transplant. They die on the transplant waiting list due to the rapid progression of the underlying disease or the consequences of the (usually unsuccessful) immunosuppressive therapy. Patients suffering from pulmonary fibrosis should therefore come to our Transplant Center at the University Hospital Zurich immediately. The waiting time for most patients is 6 to 12 months. However, this can take anywhere from a few days to years, depending on whether a suitable donor lung is available.
Both primary and secondary pulmonary hypertension (a disease characterized by an increase in vascular resistance, a rise in blood pressure in the pulmonary circulation and often subsequent right-sided heart failure) are good indications for transplantation. After the lung transplant, the right heart recovers completely within weeks.
With the advent of intravenously administered and inhaled, potent drugs, the indication for lung transplantation for this disease has become rarer. Nowadays, transplantation is only indicated for patients who do not respond to drug therapy. Nevertheless, it is advisable to present patients with a diagnosis of pulmonary hypertension to the transplant center so as not to miss the right time for inclusion on the waiting list.
Today, transplantation can be used successfully for a number of other rare lung diseases. For example, in lymphangioleiomyomatosis (cystic lung disease characterized by diffuse non-malignant proliferation of smooth muscle fibres in the wall of the lymphatic vessels): in histiocytosis X (lung disease affecting the smallest branches of the airways (bronchioles)) and sarcoidosis (granulomatous inflammation that can in principle affect any organ, but predominantly affects the lungs).
Operational procedures
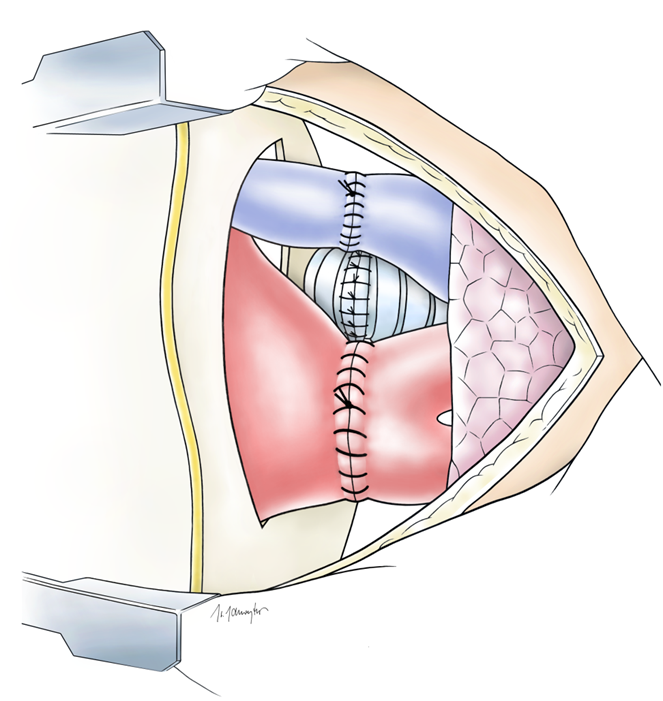
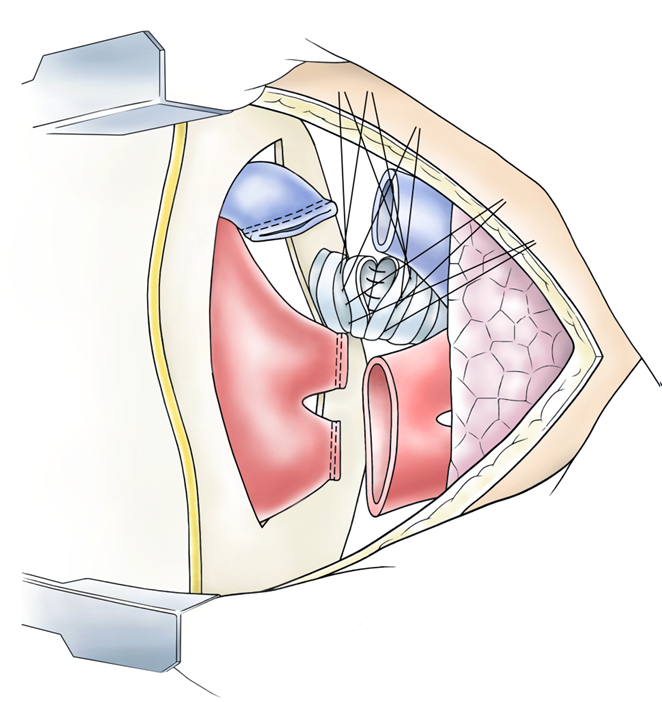
Single lung transplantation is usually performed on patients with COPD or pulmonary fibrosis. The chest is opened by means of a posterolateral thoracotomy (lateral incision along the rib), the diseased lung is removed and the donor or transplant lung is sutured to the pre-prepared main bronchus, the pulmonary artery and the pulmonary vein, or to the left atrium. During the operation, the healthy, contralateral lung is artificially ventilated. COPD rarely leads to hypoxemia (low blood oxygen levels) or hemodynamic instability (unstable blood flow), which would necessitate the use of a heart-lung machine. In contrast, this is more often the case in primary pulmonary hypertension or in patients with pulmonary fibrosis and secondary pulmonary hypertension.
Illustration Implantation der Lunge
Until the end of 2000, bilateral (bilateral) lung transplantation – often in patients with cystic fibrosis – was performed via a transverse thoracosternotomy, the so-called clamshell incision. In many cases today, this longitudinal transection of the sternum – with its higher post-transplant complication rate – can be avoided and access via a bilateral anterolateral (bilateral, anterior and lateral) thoracotomy can be chosen. And if necessary, the heart-lung machine can be used.
In combined heart-lung transplantation –themis rarely performed today and is mainly reserved for patients with congenital heart defects and Eisenmenger’s syndrome development – is accessed via a transverse thoracosternotomy or a median sternotomy (longitudinal incision of the sternum). The two organs are transplanted en bloc. Technically, the operation is classified as simpler than isolated lung transplantation. However, if previous operations have taken place, it can be significantly more complicated than an isolated lung transplant. The connection of the airways is performed as a tracheal anastomosis, the ascending aorta of the donor is connected to that of the recipient and the right atrium is connected as an atrial anastomosis. The operation is performed using a heart-lung machine.
Encouraging results
Over the past twenty years or so, lung transplantation has developed from an experimental to an established therapy for patients with advanced lung disease. This was achieved thanks to increasing experience and improved working techniques in the area of the operation itself, anesthesia, intensive care unit monitoring and new findings in immunosuppression treatment, infection prophylaxis and long-term management.
Compared to the early days of lung transplantation, the one-year survival rate has improved significantly. In an international comparison – 62% in the years 1988-1992 – the current figure is 80%. In contrast, five-year survival worldwide remained virtually unchanged at 45%, mainly due to the continued high level of chronic graft rejection. In contrast, the Zurich results show a one-year survival rate of 80%, a five-year survival rate of 65% and a twelve-year survival rate of 50%. And among patients who have undergone transplantation at the University Hospital Zurich since 1998, 87% have a one-year survival rate and 72% a five-year survival rate. Perioperative survival is over 90%.
Treatment and risks after TPL
Today, lung transplantation is considered an established and safe therapy. The time after the transplant is more critical. The specific and consistent post-transplant treatment of any inflammatory risks that may occur is crucial for long-term survival. In contrast to other transplanted solid organs such as the heart, liver or kidney, the transplanted lung is exposed to a large number of noxious substances (chemical substances and physical effects) with every breath, which is a key characteristic of the chronic transplant rejection reaction that occurs much more frequently than in other organs: the immune defense of transplanted patients is suppressed and dangerous pathogens can penetrate the organism more easily and spread there. Risk factors for chronic graft rejection are both allo-immune (e.g. acute rejection) and non-allo-immune (e.g. viruses, reflux of gastric juices into the esophagus, fungi, organic and inorganic pollutants in the outside air, etc.).
Consistent follow-up and further treatment
Post-transplant management focuses strongly on the early detection of possible damage or acute rejection of the transplanted lung, as the body perceives the new lung as a foreign body. The condition of the transplant is regularly checked using invasive and non-invasive methods such as bronchoscopy, bronchoalveolar lavage and transbronchial lung biopsies. And recommended regular lung function tests (spirometry) can also be carried out by the person concerned at home.
Diese Patientin litt an einer Zystischen Fibrose. Eine Krankheit, die ihre Lebensqualität stark einschränkte und weswegen sie unter Dauer-Sauerstoff-Therapie stand. Im 2002, damals war sie 16 Jahre alt, haben wir beide Lungen transplantiert. Seither kommt die junge Frau regelmässig zur medizinischen Kontrolle ins UniversitätsSpital. Sie ist in einem sehr guten Allgemeinzustand. Das Bild zeigt die Patientin vor der Transplantation im 2002 und zehn Jahre später während einer Motorrad-Tour gemeinsam mit ihrem Vater.
Diese Patientin litt an einer Zystischen Fibrose. Eine Krankheit, die ihre Lebensqualität stark einschränkte und weswegen sie unter Dauer-Sauerstoff-Therapie stand. Im 2002, damals war sie 16 Jahre alt, haben wir beide Lungen transplantiert. Seither kommt die junge Frau regelmässig zur medizinischen Kontrolle ins UniversitätsSpital. Sie ist in einem sehr guten Allgemeinzustand. Das Bild zeigt die Patientin vor der Transplantation im 2002 und zehn Jahre später während einer Motorrad-Tour gemeinsam mit ihrem Vater.
Ex vivo lung perfusion (EVLP)
There is still a shortage of suitable donor lungs for patients who require a lung transplant. Since 2012, donor lungs have therefore been connected to a lung perfusion system (ex vivo lung perfusion) and mechanically ventilated at our clinic after standard removal for evaluation and optimization; similar to a heart-lung machine. Lungs that previously could not be used for transplantation improve their organ function on this system for subsequent successful transplantation.
Ex-vivo lung perfusion significantly increases the number of available donor organs.
For patients
You can either register yourself or be referred by your primary care physician or gynecologist.