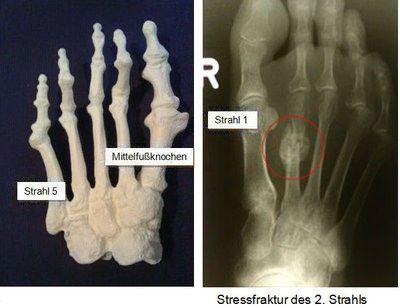
Detecting the disease
In any case, an X-ray of the foot should be taken in 2 planes. If there is no initial indication of a fracture, it makes sense to repeat the X-ray after 2 weeks, as sometimes fractures only show up on the X-ray after a delay. A purely lateral image makes diagnosis more difficult due to the overlapping of the corresponding bones. Inclined mounting makes sense here.
Fractures of the metatarsus and toes are divided into displaced fractures (fragments are widely separated) and non-displaced fractures (the shape and form of the bone is unaffected). Here too, blood circulation, motor skills and sensory perception must be checked in every case. In the area of the 5th metatarsal bone, a fracture can occur at the end close to the body, which has a special feature (Jones fracture). If the blood supply is restricted, this results in an increased rate of healing failure.
Treatment of a broken foot and toes
Conservative treatment can be carried out in the area of the 1st ray if the fracture is not displaced. A lower leg cast or a so-called Geisha shoe is applied for 6 weeks and partial weight-bearing of the corresponding extremity is recommended. If the fragments are displaced (displaced fracture), a plate is placed on the bone if the fracture occurs in the shaft area.
If the fracture is more at the ends of the metatarsal bone, wires or screws are also recommended. Any fracture that radiates into the articular surface and shows more than 2 mm of displacement must be repositioned and stabilized by surgical measures. It is important to restore the length of the 1st ray in order to avoid problems such as persistent pain in the area of the 1st ray as well as overloading damage to the other rays. In the case of fractures of rays 2 to 5, shoes with hard soles can be prescribed for non-displaced fractures and pain-adapted weight-bearing can be prescribed. If the fractures are displaced, we recommend setting the fracture (usually without opening the skin) and wearing a lower leg cast for 3 weeks. If several bones are involved, immobilization with a wire can be advantageous. This is then removed after 6 weeks. A dislocation in the nearby joints (Lisfranc joint, Chopar joint) must always be considered. These are serious injuries that require immediate surgical treatment.
In the case of a stress fracture, a lower leg cast is often applied or, as an alternative, a so-called Geisha shoe or a hard orthosis, which should be worn for 3 weeks. A full load is possible here. However, the healing process should be monitored with the help of the X-ray image. If the fracture is in the area of the 2nd ray close to the body, the cast should be worn for 6 to 8 weeks, as delayed healing rates often occur. The non-displaced fracture in the area of the 5th ray at the base (Jones fracture) can also initially be treated conservatively. A lower leg cast is recommended for 6 to 8 weeks. The lower extremity should be relieved for 4 to 6 weeks, after which partial weight-bearing can increasingly be carried out. Athletes who require faster rehabilitation in order to be able to return to training quickly may be recommended a treatment with a screw or a so-called tension bandage (wires and cerclage). If this fracture is displaced, open setting of the fracture is unavoidable. In this case, the fracture must be surgically stabilized (screw, tension belt or plate).
In the case of fractures of the toes, fixation with a wire or screw may be necessary on the first ray if the fracture is in the toe area close to the body. Otherwise, surgery in the toe area is only necessary for severely displaced fractures. Usually, broken toes are treated conservatively with the help of a plaster splint or, in many cases, only by splinting by taping to the adjacent toe (plaster toe bandage). If toes are dislocated, local anesthesia can be used to eliminate the pain and the bones can be moved into their anatomically correct position with traction and countertraction. Bruising under the nails should be relieved in good time by piercing the nail.