What are sleep-related breathing disorders?
Sleep is to a certain extent the “weak point” of breathing: Many diseases of the lungs, the cardiovascular system or the nerve-muscle system can therefore initially manifest themselves during sleep as a result of disturbed breathing. Sleep-related breathing disorders occur more frequently in cases of heart failure, COPD, obesity, neuromuscular diseases or other forms of respiratory insufficiency, for example.
For the assessment of sleep apnea or other sleep-related breathing disorders, it is therefore important to undergo a comprehensive pneumological and sleep medical examination. In addition to recording risk factors and concomitant illnesses, the quality of sleep, daily well-being and possible long-term consequences are assessed in particular. An apparative sleep examination is always required to make a diagnosis. During an initial consultation, an assessment is made as to which examination method is suitable – for example, polysomnography in the sleep laboratory, polygraphy with capnometry (carbon dioxide measurement) in the sleep laboratory or outpatient polygraphy in the home environment.
The Sleep Center of the University Hospital Zurich offers the entire spectrum of these diagnostics in pneumology. By looking at all the findings together, it can then be determined whether therapy is indicated and which form of treatment is best suited to the individual patient.
The most important treatment options include positive pressure therapies such as CPAP or ASV, which are individually adjusted in the pulmonology department. For milder forms of OSA, a customized mandibular advancement splint can be an alternative for suitable patients. If you are overweight or obese, normalizing your weight can help to improve OSA. For selected patients, surgical procedures such as a jaw repositioning osteotomy or hypoglossal nerve stimulation (“tongue pacemaker“) are also possible.
As an interdisciplinary center, the University Hospital Zurich offers these modern therapeutic approaches in collaboration with the departments of pulmonology, dentistry, ENT, oral and maxillofacial surgery and the Adipsoitas Center after careful diagnostic clarification.
Types of sleep-disordered breathing
There are four main forms, which differ in terms of their cause and pathophysiological mechanisms:
Obstructive sleep apnea (OSA/OSAS)
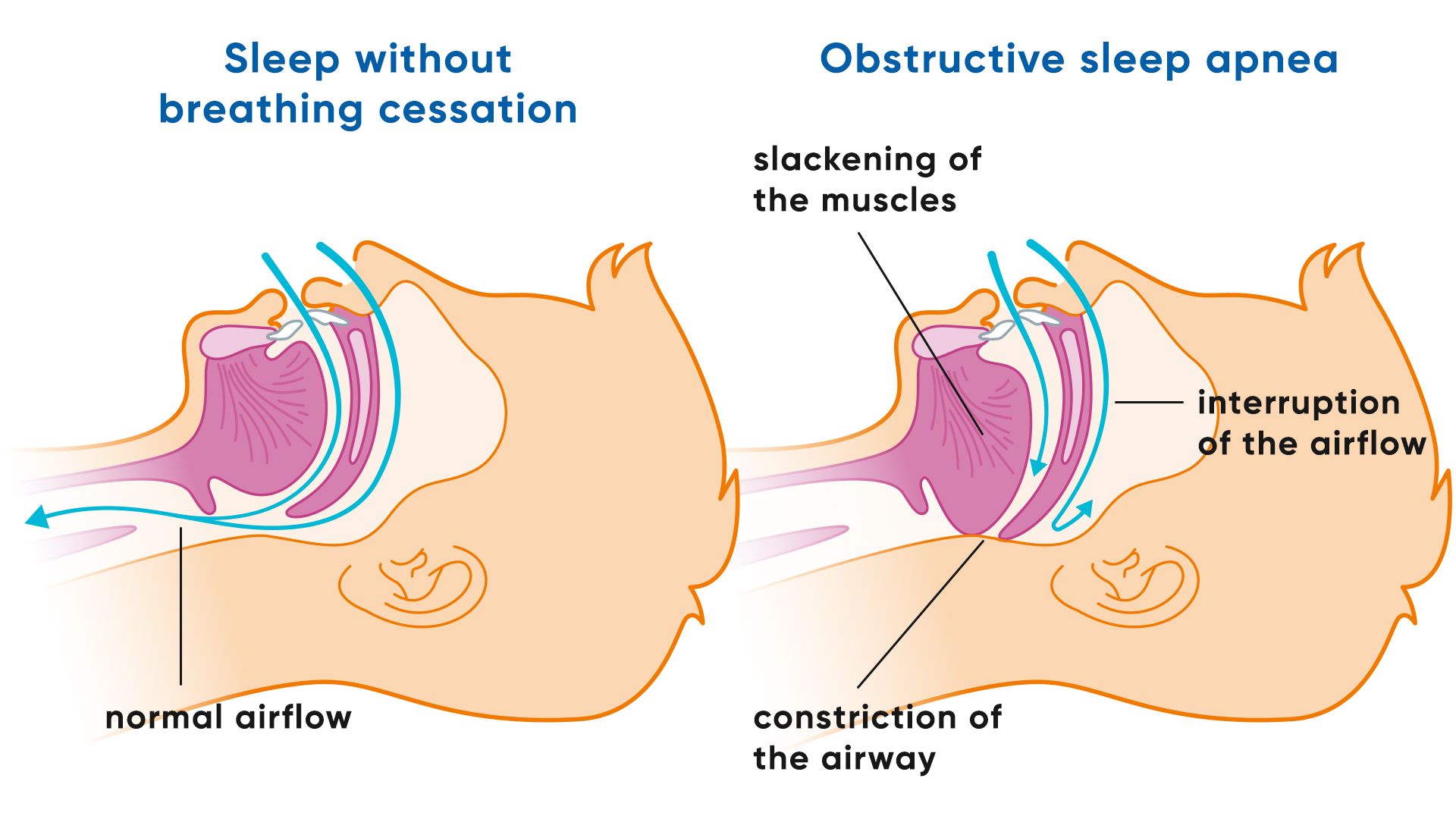
This form is caused by repeated constriction or complete collapse of the upper airway (pharynx) during sleep in patients with a narrow upper airway that is prone to collapse. This is caused by the muscles in the throat and tongue slackening at night, which obstructs or interrupts the flow of air. Typical symptoms are loud, irregular snoring, followed by pauses in breathing and subsequent audible gasps for air. Obstructive sleep apnea is by far the most common form and occurs more frequently with overweight/obesity, favorable jaw anatomy with anatomical constrictions or neuromuscular diseases.
Central sleep apnea (ZSA)
In this case, the upper airways are clear, but the respiratory drive is temporarily absent because the respiratory center in the brain does not send the corresponding signals to the respiratory muscles. As a result, respiratory movements stop completely without a mechanical blockage being present. This form is much rarer, but occurs more frequently in connection with heart failure, after strokes, when taking opiates or in certain neurological diseases.
Hypoventilation syndromes
In the case of sleep-related hypoventilation, the respiratory minute volume is permanently too low during sleep. As a result, too little carbon dioxide is exhaled, which leads to an increase in carbon dioxide in the blood and also to a lack of oxygen. The disorder often initially only occurs during sleep and can be an early sign of incipient respiratory insufficiency. Common causes are severe obesity (obesity hypoventilation syndrome), chronic lung diseases such as COPD, neuromuscular diseases or changes in the chest. Certain medications with a respiratory depressant effect can also increase hypoventilation.
Sleep-related hypoxemia
In sleep-related hypoxemia, there is a drop in the oxygen content in the blood during sleep, without the need for breathing pauses. This is usually caused by restricted oxygen uptake in the lungs or an existing respiratory disease, which becomes more noticeable during sleep. Sleep-related hypoxemia often occurs in chronic lung diseases such as COPD, interstitial lung diseases or pulmonary arterial hypertension and becomes noticeable before oxygen is also reduced during the day.
This differentiation is crucial for therapy, as both the causes and the most effective treatment approaches vary depending on the type.
Obstructive sleep apnea
Obstructive sleep apnea is characterized by repeated obstructive apneas (collapse of the upper airway during sleep) or hypopneas (partial collapse with resulting flow limitation), which lead to oxygen desaturation, sleep fragmentation (“arousals”) and cardiovascular stress. The apnea-hypopnea index (AHI), which indicates the average number of apneas and hypopneas per hour of sleep, is used to make the diagnosis. An AHI of five or more events per hour in combination with typical symptoms – such as excessive daytime sleepiness, non-restorative sleep or morning headaches – is considered diagnostically relevant. Obstructive sleep apnea can significantly impair sleep and may be associated with an increased risk of arterial hypertension, cardiovascular disease, metabolic disorders and accidents due to daytime sleepiness.
Sleep apnea frequency
Obstructive sleep apnea is one of the most common chronic diseases. Around one billion people worldwide suffer from obstructive sleep apnea.
Studies show that around 13% of men and 6% of women in middle to old age suffer from relevant obstructive sleep apnea with an indication for treatment. In women, the risk increases significantly, particularly after the menopause, which is attributed to hormonal changes.
What is obstructive sleep apnea or obstructive sleep apnea syndrome?
Obstructive sleep apnea is by far the most common form of sleep-related breathing disorder. Those affected usually snore and there is a repeated relaxation of the muscles of the throat and tongue and a collapse of the upper airway. Afterwards, those affected continue to breathe and snore again. The phase of reduced oxygen supply during the breathing cessation leads to a brief alarm reaction of the body, which is usually not consciously perceived by the person affected. Sleep is briefly fragmented (arousal) and muscle tone returns until apnea occurs again. This is not only associated with a drop in oxygen levels and sleep fragmentation, but often also with stress for the cardiovascular system (heart rate fluctuations, increase in blood pressure, etc.). If this process takes place countless times during the night, sleep is significantly disturbed. Those affected are often not rested the next morning. However, many patients suffering from symptomatic obstructive sleep apnea do not necessarily have an increased tendency to fall asleep (increased daytime sleepiness is referred to as sleep apnea syndrome), but suffer from tiredness, concentration problems, fatigue or interrupted sleep of poor quality.
Obstructive sleep apnea: causes and risk factors
In obstructive sleep apnea, the muscles of the upper airways slacken during sleep, causing them to collapse and resulting in snoring noises. A partial or complete blockage (obstruction) of the flaccid airways is responsible for the interruptions. As a result, the body is no longer supplied with sufficient oxygen, the carbon dioxide content in the blood rises and the pulse slows down. Finally, the respiratory center in the brain reacts and sounds the alarm, so to speak. The body reacts to stress:
- The airways open up again due to the tension
- Breathing resumes with rapid, deep breaths
- The affected person briefly switches to a light waking state,
- Heart rate and blood pressure increase and the body is supplied with sufficient oxygen again.
The brief waking moments are usually not consciously noticed, but they prevent restful deep sleep from taking place. The unconscious awakening is also called arousal. So if you feel constantly tired during the day and your environment tells you that you snore at night, then obstructive sleep apnea is suspected. To be sure, your relatives can observe the frequency of the interruptions. The cessation of breathing in sleep apnea occurs at least five times within an hour and lasts at least ten seconds each time.
It is estimated that around fifteen percent of middle-aged people are affected by this disease, and the number of sufferers increases with age. There are a few risk factors that can contribute to obstructive sleep apnea. These include:
- Overweight(adipostas)
- Malposition of the lower jaw (retrognathia)
- Secondary diseases such as heart failure or respiratory muscle weakness and many others
- enlarged adenoids, nasal polyps
- Alcohol, nicotine, drug consumption, sleeping pills
Diabetes mellitus, heart failure or sleeping on your back can also contribute to obstructive sleep apnea. Sleep apnea is more common in people with cardiovascular disease than in otherwise healthy people.
Symptoms of obstructive sleep apnea
As a rule, people with obstructive sleep apnea are snorers. Snoring in itself (without obstructive sleep apnea) is harmless and does not necessarily have a pathological value. However, if the relatives notice the typical breathing interruptions during sleep, then sleep apnea is suspected. Those affected often complain of tiredness during the day and sometimes have difficulty concentrating. Other symptoms may occur:
- Increased tendency to fall asleep in monotonous situations
- Fragmented sleep
- Unrestful sleep
- Headache in the morning
- Dry mouth
- Waking up in the night with shortness of breath and palpitations
- Sweating at night
- Potency problems
Even if those affected do not consciously experience the waking phases, many complain of restless sleep. Sleep disorders can cause depressive moods and even depression. It is usually relatives who urge the person concerned to see a doctor or hospital because of their own disturbed sleep.
Obstructive sleep apnea can also be a hindrance at work, because in Switzerland, for example, all driving license categories require that no illnesses with increased daytime sleepiness are present. This is another reason not to take nightly breathing interruptions lightly, but to have a thorough medical examination.
In addition, obstructive sleep apnea is an important risk factor for high blood pressure, especially nocturnal high blood pressure or so-called therapy-resistant arterial hypertension, which does not respond well to blood pressure-lowering medication. Obstructive sleep apnea can also promote atrial fibrillation.
Special features of obstructive sleep apnea in men and women
In men, obstructive sleep apnea (OSA) is more common with the classic leading symptoms such as loud, irregular snoring, interrupted breathing and significant daytime sleepiness.
Women, on the other hand, more often report non-specific or atypical complaints such as difficulty falling asleep or sleeping through the night, morning headaches, mood swings, depressive moods or concentration problems. In addition, breathing stops occur more frequently in REM sleep phases, which can make diagnosis more difficult.
These differences in symptoms require gender-sensitive diagnostics in order to avoid misdiagnosis and enable early, targeted therapy. Sleep apnea also presents differently in sleep studies. Women, especially premenopausal women, are more likely to have hypopneas (partial collapse) with “arousals” and without significant oxygen desaturations, so that polysomnography is necessary for diagnosis and polygraphy in the home environment is often not sensitive enough. Obstructive sleep apnea, which mainly occurs during dream sleep, is also more common in women. The symptoms and consequences do not necessarily correlate with the apnea-hypopnea index. Even an apnea-hypopnea index that is not significantly elevated can lead to symptoms or a patient with a significantly elevated apnea-hypopnea index can be largely symptom-free. Polysomnographies or polygraphs measure much more than the apnea-hypopnea index and in particular also assess oxygen deficiency and autonomic stress.
Diagnosis of obstructive sleep apnea syndrome
To make an initial diagnosis, we will take a medical history, possible symptoms incl. Record observations of relatives and risk factors (medical history and examination). During the physical examination, the patient’s weight, height, blood pressure, heart and lungs are examined. A blood test can show whether there is a thyroid dysfunction and whether the number of red blood cells has increased due to the lack of oxygen in a longstanding sleep apnea. An arterial blood gas analysis provides information about the oxygen and carbon dioxide content. The physical diagnosis can be followed by an examination of breathing and sleep.
Portable measuring device for sleep apnea
There are various ways of examining breathing during sleep. Various parameters can be checked using a portable polygraph device that you can take home with you. Put the probes on before you go to bed. While you sleep, your breathing, heart rate and blood oxygen saturation are measured. The probes also register body position and snoring noises. If the suspicion of OSA is confirmed, treatment or further examination in a sleep laboratory may be advisable. However, this method is only suitable if there is a high pre-test probability of severe obstructive sleep apnea with cyclical oxygen desaturation. It is not suitable for patients with pulmonary or cardiovascular diseases or other sleep disorders (e.g. insomnia) and is less sensitive in detecting obstructive sleep apnea (especially in women).
OSA: Sleep laboratory
During an examination in the sleep laboratory, your sleep can be observed in detail and recorded using various measuring devices. In the evening, you will move into a special single sleep laboratory room equipped with a video camera and recording devices. In addition to the pulse rate and oxygen content, sensors are used to record breathing movements, limb and eye movements and, in the case of polysomnography, brain waves. The frequency of apneas and hypopneas per hour is calculated from the number of complete and partial pauses in breathing as the apnea-hypopnea index (AHI). The AHI is a measure of the severity of obstructive sleep apnea If (additional) central sleep apnea or hypoventilation is suspected, an examination in the sleep laboratory including carbon dioxide measurement (capnometry) is indicated.
Obstructive sleep apnea syndrome: prevention, early detection, progression
To a certain extent, you can try to prevent obstructive sleep apnea. First of all, this includes checking the weight. Excessive obesity promotes breathing stops, partly because too much abdominal fat and fat on the neck makes breathing more difficult. Make sure you eat a balanced, healthy diet with plenty of fruit, vegetables and fiber. Go easy on sugar, control the fats you consume – plant-based are better than animal-based – and be a little stingy with carbohydrates. Exercise also helps to achieve a healthy normal weight: leave the car at home and take the bike, don’t take the elevator, take the stairs instead. If you stop smoking and avoid alcohol and sleeping pills before going to bed, this also reduces the risk of sleep apnea.
Further everyday tips against sleep apnea
In addition to weight reduction, a healthy diet and abstaining from alcohol, nicotine and sleeping pills, certain habits and exercises can have a supportive effect:
- Optimize sleep hygiene: Regular sleeping times, a quiet, dark bedroom and avoiding screen use just before sleep promote restful sleep.
- Train changes in position: Sleeping on your side reduces the frequency of breathing interruptions for many sufferers. Positioning aids or special side sleeping pillows are helpful.
Breathing and tongue muscle training: Short daily exercises to strengthen the tongue and throat muscles can reduce the collapse of the upper airways (e.g. consciously pressing the tongue against the palate, humming sounds).
- Regular physical activity: Endurance sports such as walking, cycling or swimming improve general fitness and support respiratory function.
- Promote nasal breathing: If you have a chronically blocked nose, treatment or targeted nasal breathing training can improve breathing at night.
These measures do not replace medical therapy, but can support treatment and improve quality of life.
Course of obstructive sleep apnea
React soon if your partner complains about your loud snoring at night. Do not accept daytime tiredness as an annoying evil, but visit us to find out the cause. A diagnosis of obstructive sleep apnea or obstructive sleep apnea syndrome and treatment can help you regain a better quality of life and avert possible consequences such as high blood pressure, heart attacks and strokes.
If left untreated, the hundreds of breathing interruptions during the night can
cause. Daytime tiredness makes driving risky, which is particularly dangerous for professional drivers. Drowsiness during the day can lead to incapacity to work. In people with dementia, untreated sleep apnea increases cognitive decline.
Self-help groups
The exchange with people who are affected by the same disease can be a great support in coping with the disease. Advice on finding a suitable self-help group is available from Selbsthilfe Zürich. Self-Help Zurich and the University Hospital Zurich are cooperation partners in the national project “Health literacy thanks to self-help-friendly hospitals”.
Treating obstructive sleep apnea
Targeted therapy can significantly improve the quality of life and considerably reduce the risk of secondary diseases such as arterial hypertension, heart attack or stroke. Various approaches are available depending on the severity and individual requirements.
- General measures include weight reduction, abstaining from alcohol, smoking and sedative medication, as well as a preferred side position (avoidance of supine position) during sleep. These changes can significantly reduce the frequency of breathing stops, especially in milder forms.
- CPAP therapy(Continuous Positive Airway Pressure) is the standard treatment for obstructive sleep apnea. A continuous positive pressure is supplied via a mask, which keeps the airways open and reliably prevents apnea.
- Individually adapted mandibular advancement splints or position-changing vibration systems can be used as technical aids – especially for milder forms or if CPAP is not tolerated.
- Surgical procedures can be useful if there are anatomical constrictions, for example due to enlarged palatine or pharyngeal tonsils, nasal polyps or malpositioned jaws.
The choice of therapy is always individual and can be found in detail on the special treatment page.
Frequently asked questions about sleep apnea
A complete cure is not possible in most cases. Mild forms can improve significantly by reducing weight, changing sleeping habits or treating anatomical causes. For many patients, however, long-term therapy – e.g. with CPAP – is necessary to reliably prevent breathing stops.
With adequate treatment, life expectancy is not limited. However, if left untreated, severe obstructive sleep apnea can increase the risk of cardiovascular disease, metabolic disorders and accidents, which has a long-term negative impact on life expectancy.
Not every form of obstructive sleep apnea is dangerous or needs to be treated. Severe obstructive sleep apnea, especially if it leads to severe oxygen desaturation or cardiovascular stress, can be dangerous. Repeated interruptions in breathing at night lead to a lack of oxygen, a rise in blood pressure and an increased release of stress hormones. In the long term, the risk of high blood pressure, heart attack, stroke, cardiac arrhythmia and daytime tiredness increases, with an increased risk of accidents.
CPAP therapy keeps the upper airways open by means of continuous positive pressure, prevents apnea and normalizes the oxygen supply. Alternatives are mandibular advancement splints, position modification systems or – in special cases – surgical interventions such as hypoglossal nerve stimulation or jaw repositioning osteotomy
With portable polygraphy devices, respiratory flow, respiratory effort, oxygen saturation, heart rate and sleep position can be recorded at home and a diagnosis can be made if there is a high pre-test probability of moderate to severe obstructive sleep apnea of the classic type (with relevant oxygen desaturations). However, the diagnosis must be confirmed by a medical evaluation of the sleep study. A home examination is not suitable for ruling out sleep apnea. If necessary, an examination in a sleep laboratory is required in a second step.
The choice of mask depends on individual factors such as anatomy, sleeping position and personal comfort. There are nasal masks, nasal cushion masks and mouth-nose masks; the most suitable variant is tested as part of the therapy fitting.
In addition to obstructive sleep apnea (the most common form), there are also various forms of central sleep apnea (less common) and combined forms of obstructive and central sleep apnea. Other forms of sleep-related breathing disorders are hypoventilation (e.g. obesity hypoventilation syndrome) and hypoxemia. There are also special forms of obstructive sleep apnea such as REM-dominant obstructive sleep apnea, supine-dominant obstructive sleep apnea or upper airway resistance syndrome (UARS) and obstructive sleep apnea can occur together with another form of sleep-related breathing disorder
In addition to established methods such as CPAP, modern approaches such as hypoglossal nerve stimulation or individualized, digitally controlled mandibular advancement splints are also used. Research and technology are continuously developing further patient-specific solutions.
Typical signs are loud, irregular snoring, observed breathing interruptions, frequent nocturnal awakenings with shortness of breath and pronounced daytime sleepiness. A reliable diagnosis can only be made through a medical examination.
The most common symptoms include loud snoring, breathing interruptions during sleep, morning headaches, unrefreshing sleep, fragmented sleep, concentration problems, daytime tiredness, mood swings and reduced performance. Some sufferers also report dry mouth, night sweats or palpitations.

