Diagnosis
Some patients suffer from dyspnea, angina pectoris and syncope, while others remain largely asymptomatic. HOCM is associated with an increased risk of sudden cardiac death, especially in younger patients; it is one of the most common causes of death in trained young adults. The elongated and somewhat abnormally positioned subvalvular apparatus of the mitral valve is displaced into the outflow tract during systole. This late-onset distortion of the mitral valve leads to severe mitral valve insufficiency, which can be the main cause of the symptoms.
Echocardiography should describe not only the severity but also the extent of the obstruction (subvalvular, mid-ventricular, apical) and the presence of systolic anterior motion of the mitral valve. If neither a systolic anterior motion nor a resting gradient is present, a provocation test with Valsalva Maneuver or a pharmacological load (amyl nitrite) should be performed. A cardiovascular magnetic resonance examination (CMR) is recommended in all cases, as this examination provides detailed information on cardiac morphology, ventricular function and even specific characteristics of the myocardial tissue.
Drug treatment
Drug therapy is indicated for mild forms of obstruction and oligo-symptomatic patients. If the obstruction is more severe, with or without symptoms, the aim should be to remove the obstruction. This must be completely rectified. To this end, affected patients should – if necessary – strive to make lifestyle changes.
Surgical treatment
The purpose of resection of the septal musculature is to free the left ventricular outflow tract from the hypertrophic musculature. The procedure is performed through an access in the aorta and through the aortic valve. The results of surgical subvalvular myectomy depend largely on the experience of the surgeon and the entire team. In institutions with a high level of expertise, a mortality rate of 1% can be expected. The most common complications are total a-v block, inadequate resection with or without relevant mitral valve insufficiency. In individual cases, the latter must be reconstructed in the same session or, exceptionally, replaced.
The long-term results after resection of hypertrophic cardiomyopathy are generally very good. A small percentage of patients with early postoperative blocking AV conduction disorders will require a pacemaker before leaving hospital.
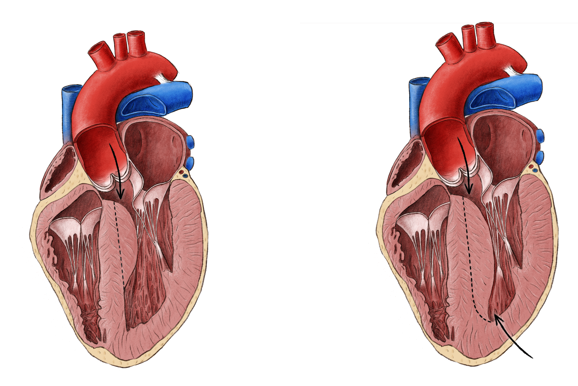
Resection in hypertrophic obstructive cardiomyopathy (left through the aortic valve in the case of limited severity, right through both the aortic valve and the tip of the left ventricle in the case of severe severity)