What are anal fistulas?
Anal fistulas are unnatural ducts that form between the anal canal and the skin around the anal opening. The ducts usually form due to inflammation of special glands in the anal canal, the proctodeal glands. In humans today, they are only incompletely and individually present in varying numbers. They may even be missing altogether. However, there are other causes of anal fistulas, for example chronic inflammatory bowel diseases such as Crohn’s disease and ulcerative colitis.
A fistula in the anal area can be very uncomfortable: Those affected usually feel pain and secretions flow out of the opening of the fistula. In addition, the area around the fistula may become red and swollen due to the inflammation.
Anal fistulas often form as a result of an anal abscess due to a purulent inflammation caused by bacteria. Anal fistula and anal abscess are actually the same clinical picture. The anal abscess is accompanied by an encapsulated accumulation of pus and corresponds to the acute form. Anal fistula, on the other hand, is the chronic variant in which the purulent fluid seeps out through an opening in the skin.
Anal fistulas usually do not heal by themselves. The treatment usually consists of surgery, for which there are various techniques. Which of these doctors choose depends on the type and course of the fistula. Without surgical treatment, there is a risk that the fistula will become inflamed and pus will form. And the well-being and quality of life of those affected also suffer.
Anal fistulas – frequency and age
Anal fistulas are relatively common. Experts estimate that around 20 out of every 100,000 inhabitants contract the disease every year. The frequency seems to vary within Europe, as a study from 2007 showed: the population in Spain developed anal fistulas the least frequently (1.04 per 10,000 inhabitants/year). The highest rate was in Italy (2.32 per 10,000 inhabitants/year).
The unnatural ducts in the anal region around the sphincter muscle mainly affect adults between the ages of 30 and 50. Men are significantly more frequently affected due to the increased number of proctodeal glands.
Anal fistulas: Causes and risk factors
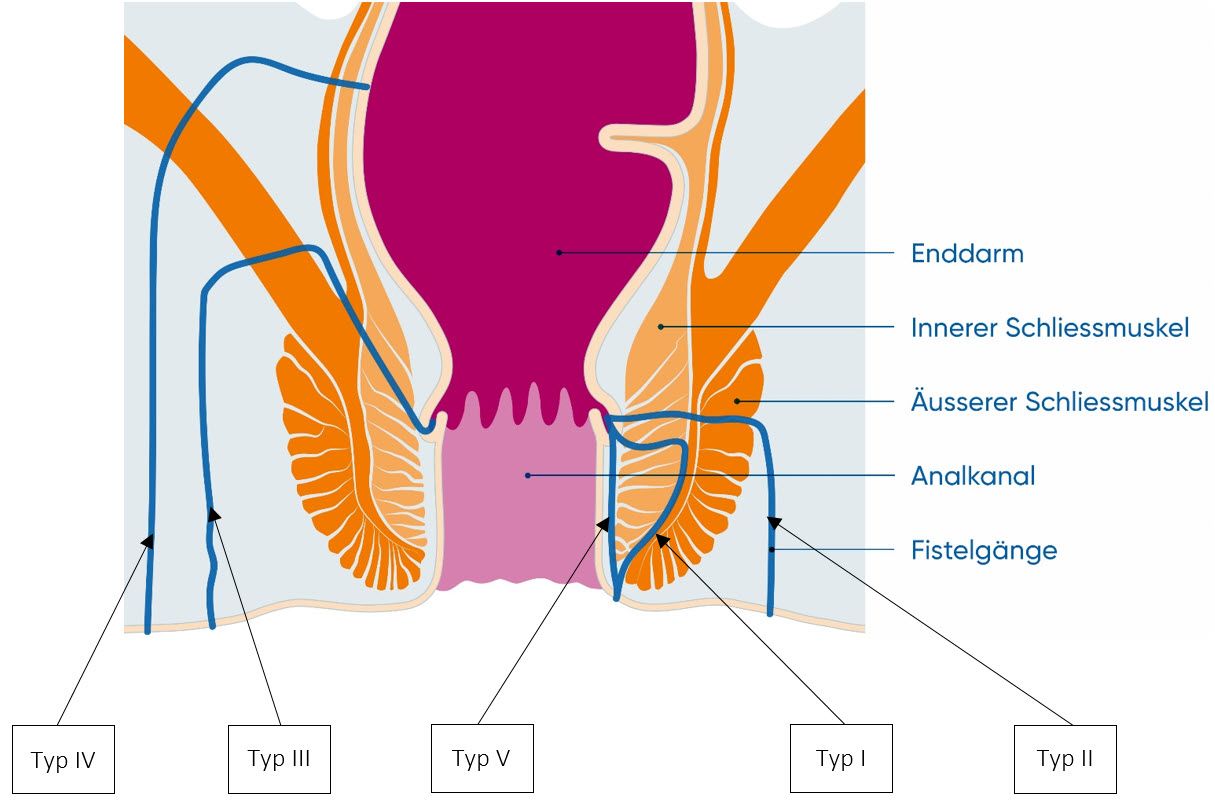
The most common cause of anal fistulas is an infection of the proctodeal glands with bacteria. The inflamed glands eventually become a long duct and a fistula. Anal fistulas can make their way to the surface of the skin in very different ways and take different courses. According to the Parks classification, anal fistulas are divided into five different types – depending on their course in relation to the sphincter muscle (Musculus sphinkter ani):
- Intersphincteric anal fistulas (type I) are very common. The ducts run between the internal and external sphincter.
- Transsphincteric anal fistulas (type II) are common. The ducts penetrate both sphincters completely, i.e. both the inner and outer parts.
- Suprasphincteric anal fistulas (type III) are rare. The ducts run between the sphincter and the pelvic floor muscles.
- Extra-sphincteric anal fistulas (type IV) are very rare. The fistula tracts do not involve the sphincter muscle and originate outside the anal canal.
- Submucosal (subanodermal) anal fistulas (type V) run directly under the mucous membrane and do not affect the sphincter muscle.
Risk factors for anal fistulas
According to recent findings, there are a number of risk factors that are thought to promote anal fistulas. These include, for example:
- Obesity
- Diabetes (diabetes mellitus)
- Dyslipidemia
- Skin diseases
- High consumption of very spicy foods
- High daily salt consumption
- Smoking
- Alcohol consumption
- Lack of exercise, prolonged sitting
- Prolonged sitting on the toilet during bowel movements
- psychosocial stress
Anal fistula symptoms
Anal fistulas can cause some very unpleasant symptoms. The following complaints are possible:
- Pain, especially when sitting and during bowel movements
- Secretions, which may contain pus, persistently leak from the fistula. Patients may feel disturbed by the unpleasant odor and oozing that contaminates the underwear.
- Bleeding
- Itching
- Symptoms of inflammation: Fever as well as redness, overheating and swelling of the anal region
- If the fistula is very large, wind or stool may escape.
Do not be afraid to consult a doctor if you experience such symptoms, as a fistula does not usually disappear by itself.
Anal fistulas: Diagnosis with us
The diagnosis of an anal fistula always begins with a medical history interview. The doctor will ask you a few questions, for example:
- What are your symptoms? e.g. pain, secretion in the anal region
- When did the complaints first appear?
- How intensively are they pronounced?
- Do the symptoms improve from time to time or do they persist?
- Do you have any known diseases? e.g. chronic inflammatory bowel disease, HIV, infections, cancer
- Lifestyle: What do you eat and how much do you exercise? Are you a smoker? How much alcohol do you drink?
- Previous operations: Have you ever had surgery in the anal region or have you had diseases in this area? If so, which one?
Doctors can usually draw conclusions from your answers as to whether it could be an anal fistula.
State-of-the-art diagnostics and treatment
At the USZ, we offer the entire spectrum of treatment for proctological diseases. We work in an interdisciplinary manner with various clinics and centers and offer state-of-the-art diagnostics and treatment. We are one of two centers in Switzerland offering stem cell treatment for perianal fistulas caused by Crohn’s disease.
Anal fistulas: Prevention, early detection, prognosis
The cause of anal fistulas is in most cases an inflammation of the proctodeal glands. And you cannot prevent this. In the case of other diseases such as Crohn’s disease or cancer, you also have few options for prevention. You may be able to start with a healthy lifestyle, as some factors seem to favor anal fistulas. Some tips:
- Move as much as possible in everyday life and exercise.
- If your job requires you to spend a lot of time sitting down, make sure you get enough exercise in between.
- Make sure you eat a healthy diet with plenty of fruit, vegetables and wholegrain products. Use salt sparingly and be careful with spicy foods.
- Give up smoking.
- Only drink alcohol in moderation and take regular alcohol breaks.
No special measures for the early detection of anal fistulas are known. Always consult your doctor if you notice pain or purulent secretions in the anal region. This prevents repeated inflammation and purulent abscesses from forming and the anal fistula from becoming chronic.
Course and prognosis of an anal fistula
Anal fistulas do not normally heal by themselves. In most cases, surgery is required to achieve definitive closure of the fistula.
The consequences can be repeated inflammations and anal abscesses. Anal fistulas can also affect the rectum. In up to a third of cases, the sphincter muscle in the anus is damaged, resulting in more or less severe fecal incontinence. Even after an operation in which doctors split the fistula (fistulotomy), the risk of fecal incontinence can be increased if the sphincter muscle did not function properly beforehand. A rarity is the formation of fistula cancer or fistula carcinoma in the case of very long existing fistulas.
Anal fistulas: Treatment by surgery
Treatment of anal fistula consists of surgery. Only very rarely does it heal without therapy. There are several surgical techniques. The method surgeons use depends on the type of anal fistula, its course and especially in relation to the sphincter. The aim is always to preserve the function of the sphincter and to heal the anal fistula permanently.