Overview: What is ulcerative colitis?
Ulcerative colitis is a chronic inflammatory bowel disease. Typically, the disease often progresses in phases, alternating between symptom-free periods and bouts of inflammation. Ulcerative colitis only affects the large intestine and remains limited to the uppermost layer of the intestinal wall, namely the intestinal mucosa. Ulcers” form there, i.e. wounds and shallow defects in the mucous membrane. The Latin term “ulcus” means “ulcer”, while “colitis” stands for an inflammation of the large intestine (colon). This is where ulcerative colitis gets its name from.
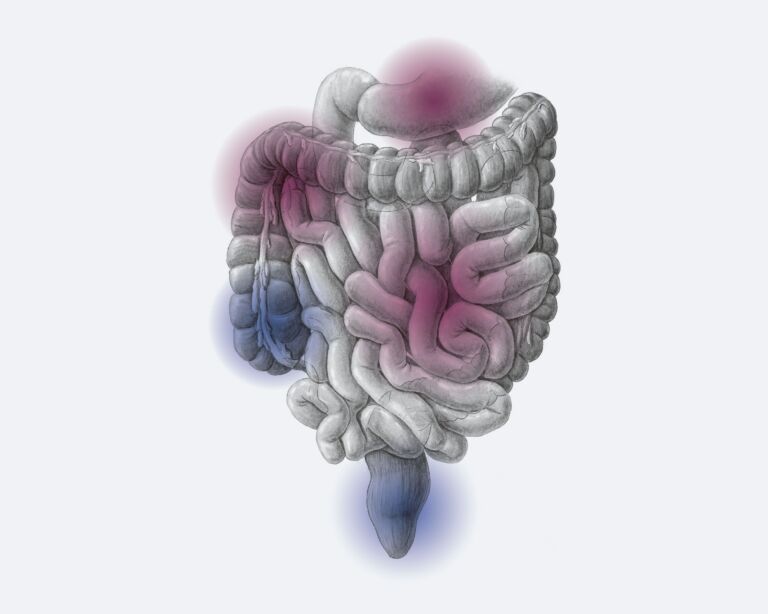
Ulcerative colitis always begins in the last section of the large intestine, the rectum, and is at its worst there. From there it can spread to other areas of the colon to varying degrees. In severe cases, it can even affect the entire colon.
Like Crohn’s disease, ulcerative colitis is a chronic inflammatory bowel disease (IBD). They are the most important main representatives that doctors summarize under the collective term IBD or IBD.
Ulcerative colitis – frequency and age
Chronic inflammatory bowel disease (IBD) is one of the most common diseases in Switzerland: Around one in 350 people suffer from it. This corresponds to more than 25,000 people. Men and women suffer from ulcerative colitis at roughly the same rate. The disease usually manifests itself for the first time in young adults between the ages of 25 and 35. However, younger people such as small children or senior citizens can also fall ill. A “senile colitis” is also known, which occurs in elderly people.
Differences in Crohn’s disease
Like Crohn’s disease, ulcerative colitis is a chronic inflammatory bowel disease. Even though the symptoms such as diarrhea and abdominal pain are very similar in both diseases, there are some differences. Crohn’s disease is characterized by the following features:
- The disease can affect the entire gastrointestinal tract – from the mouth to the anus.
- The foci of inflammation are not connected, but can occur in different parts of the intestine. There are always healthy sections of intestine in between.
- The inflammation usually affects all layers of the intestinal wall, not just the superficial intestinal mucosa. The inflammation therefore penetrates much deeper into the intestinal layers.
- In half of those affected, short-circuit connections from bowel to bowel or from bowel to skin, so-called “fistulas”, form in the course of the disease.
More about the intestinal organ
Therapy by specialists
Ulcerative colitis is a chronic inflammation of the colon that occurs in episodes and requires a graded treatment approach. In the majority of cases, the disease can be successfully controlled with drug therapy, which the gastroenterologist finds together with the patient and adjusts during the course of the disease. Only in rare and severe cases with no or insufficient response to drug therapy, surgical therapy may be the best solution. At the USZ, there is a team of proven specialists with many years of experience in the medicinal and surgical treatment of ulcerative colitis.
Ulcerative colitis: causes and risk factors
The causes of ulcerative colitis have not yet been clarified. However, researchers believe that several factors must be at work for the inflammatory bowel disease to develop.
Possible triggers that play a role in its development are:
- Altered intestinal mucosa: In people with ulcerative colitis, the protective mucus layer on the intestinal mucosa is often thinner than in healthy people. Its defense function is impaired and it has less resistance to pathogenic germs. This makes it easier for bacteria to overcome the (normally protective) intestinal barrier and penetrate the intestinal mucosa. The immune system sends out defense patrols and inflammation occurs.
- Genes: Ulcerative colitis occurs more frequently in some families. This suggests that hereditary factors are involved. The risk of contracting the disease is higher for close relatives. However, genetic predisposition plays a lesser role in colitis than in Crohn’s disease and is only relevant for one in ten cases.
- Environmental factors: Researchers are discussing environmental factors and improved hygiene standards as possible contributors because disease rates are climbing in Western industrialized countries and are also rising sharply in countries adopting Western lifestyles, such as in urban China.
Symptoms of ulcerative colitis
Ulcerative colitis can cause unpleasant symptoms during an acute flare-up. The more extensive the inflammation, the more pronounced the symptoms can be.
Possible symptoms of ulcerative colitis:
- Diarrhea, which is often bloody and/or slimy
- Abdominal pain or abdominal cramps, often in the left lower abdomen
- Frequent urge to defecate and the feeling of having to defecate, sometimes very urgently and sometimes uncontrollably
- Nocturnal bowel movements, frequent bowel movements of up to 20 times a day
- Pain before or after a bowel movement
- Feeling of being “bloated”
- Loss of appetite
- Weight loss
- Tiredness and fatigue
- Reduced performance, physical weakness
- Fever
- Anemia and iron deficiency due to blood loss with bowel movements
Diagnosis ulcerative colitis
We will first ask you a few questions about your medical history (anamnesis) to get a first impression. Some examples:
- What exactly are the symptoms you suffer from? Abdominal cramps, blood and mucus in your stool?
- How often do you have diarrhea, how often is blood mixed in and do the bowel movements also occur at night?
- How long have the symptoms been present and how severe are they?
- Are there periods without complaints in between?
- Do you have any known illnesses, such as an intestinal infection, food intolerance or food allergy?
- Are you taking any medications? If yes: Which and since when?
- Do you have a family history of chronic inflammatory bowel disease? Parents, siblings?
These and other questions help us to make an initial assessment. This is followed by further examinations to differentiate ulcerative colitis from Crohn’s disease or other diseases.
Other diagnostic methods
The diagnosis of ulcerative colitis can often be made after these examinations. Sometimes further diagnostic methods are used if the result is inconclusive. These include, for example, magnetic resonance imaging (MRI) or endoscopy of the esophagus, stomach and duodenum. It is called esophagogastroduodenoscopy.
Ulcerative colitis: prevention, early detection, prognosis
The causes of ulcerative colitis are not yet known. It is therefore not possible to effectively prevent the intestinal disease. Breastfeeding appears to reduce the risk of ulcerative colitis to a certain extent. Babies who were breastfed for at least six months are less likely to develop bowel disease than “bottle-fed” babies. It has not yet been proven whether the diet has a protective effect.
In ulcerative colitis, early detection plays a role in that sufferers have an increased risk of colorectal cancer. In general, it can be said that ulcerative colitis that is discovered in good time can often be treated more effectively. This reduces the risk of possible complications.
Course and prognosis of ulcerative colitis
Ulcerative colitis is a disease that usually progresses in phases. Phases in which the disease is active alternate with symptom-free periods. How often these flare-ups occur and how intense they are varies from person to person and of course depends on the correct and individually adapted therapy. Some people only experience a few flare-ups in the course of their lives, while others get them several times a year. Sometimes the bowel remains severely inflamed for a long time. In this case, surgical removal of the colon is the correct and necessary measure. Fortunately, thanks to improved medication, this is now only the case for less than one in ten people affected in Switzerland.
It is important that you receive adequate treatment for ulcerative colitis. You should also undergo regular examinations for the early detection of bowel cancer. Life expectancy is then similar to that of the normal population.
Complications of ulcerative colitis
As the disease progresses and the ulcerative colitis spreads, some complications can develop. Sometimes an acute attack of the disease is particularly severe. Doctors speak of “fulminant colitis”. These complications are possible with ulcerative colitis:
- Toxic megacolon: This is a severe inflammation of the entire intestinal wall, which causes the intestine to stretch considerably – the intestine can rupture, which is life-threatening. We have to operate immediately.
- Intestinal rupture: This is life-threatening and requires rapid surgery.
- Intestinal bleeding: They can be caused by severe inflammation. In severe cases, surgery is sometimes necessary.
- Colorectal cancer: People with ulcerative colitis have an increased risk of colorectal cancer, which is why you should undergo regular cancer screening. The most important measure is a colonoscopy. This enables us to detect and treat precancerous lesions or bowel cancer in good time. Discuss with your doctor at what intervals it makes sense to have a colonoscopy. Your personal risk of bowel cancer depends, for example, on how extensive and severe the inflammation is, whether close family members have had bowel cancer, whether you have already been diagnosed with precancerous bowel lesions or whether you have other risk factors for bowel cancer (e.g. chronic inflammation of the bile ducts, primary sclerosing cholangitis).
Self-help groups
The exchange with people who are affected by the same disease can be a great support in coping with the disease. Advice on finding a suitable self-help group is available from Selbsthilfe Zürich. Self-Help Zurich and the University Hospital Zurich are cooperation partners in the national project “Health literacy thanks to self-help-friendly hospitals”.
Ulcerative colitis: treatment with different strategies
Ulcerative colitis is a chronic disease that cannot be cured, but can usually be treated very well. It is important that experts are consulted for treatment. We usually combine several treatment approaches to increase effectiveness. The therapies are intended to reduce inflammation, alleviate symptoms, prevent new relapses, extend the time between two relapses, and prevent complications and late effects. This often allows for a symptom-free everyday life with a good quality of life. As a rule, you can also pursue your profession.