What are the functions of the intestine?
The intestine is just as important for the immune system as it is for digestion. In the three to four meter long small intestine, digestive juices “break down” the food. Proteins, fats and carbohydrates as well as minerals and vitamins are absorbed here. This is done with the help of digestive juices.
The large intestine extracts the water from the food pulp and thickens what is left. It also harbors trillions of bacteria that produce useful substances.
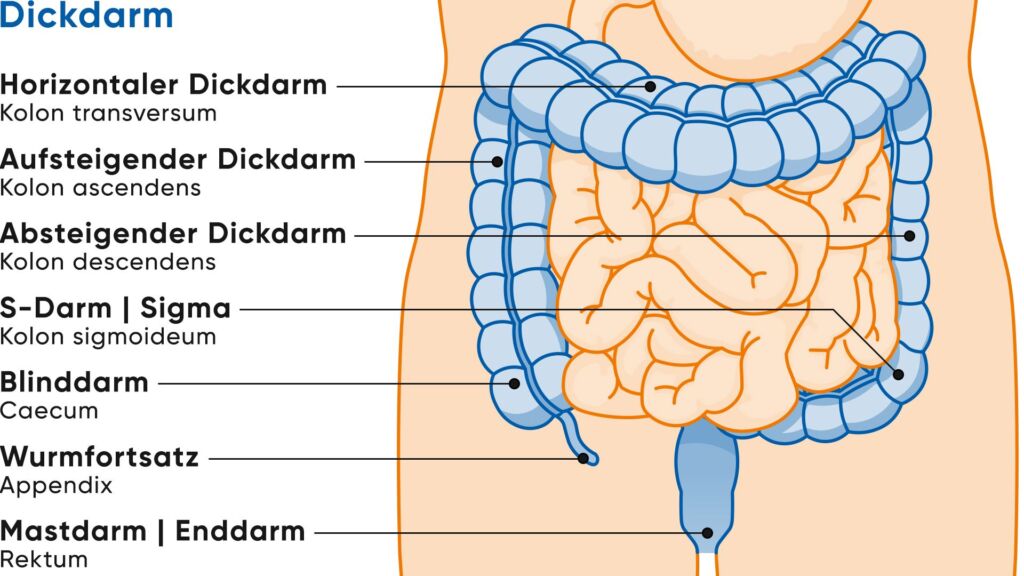
Anatomically, the large intestine consists of several parts:
- Cecum: a short piece of intestine that lies in the lower right side of the abdomen and ends blindly. The “appendix vermiformis”, a small appendage, originates there.
- Large intestine (colon), consisting of ascending colon, transverse colon, descending colon and sigmoid
- Rectum
Intestine - structure, function, diseases
The intestine is an important part of our digestive system, which consists of two main parts: The small intestine and the large intestine. It processes the food we eat every day and absorbs the nutrients. It also ensures that harmful substances are excreted.
How common is colorectal cancer?
In Switzerland, more than 4,000 people are diagnosed with colorectal cancer every year. In this country, almost five out of every 100 women will be affected in the course of their lives, and about six out of every 100 men. Colon cancer is thus one of the most common tumor diseases in both sexes.
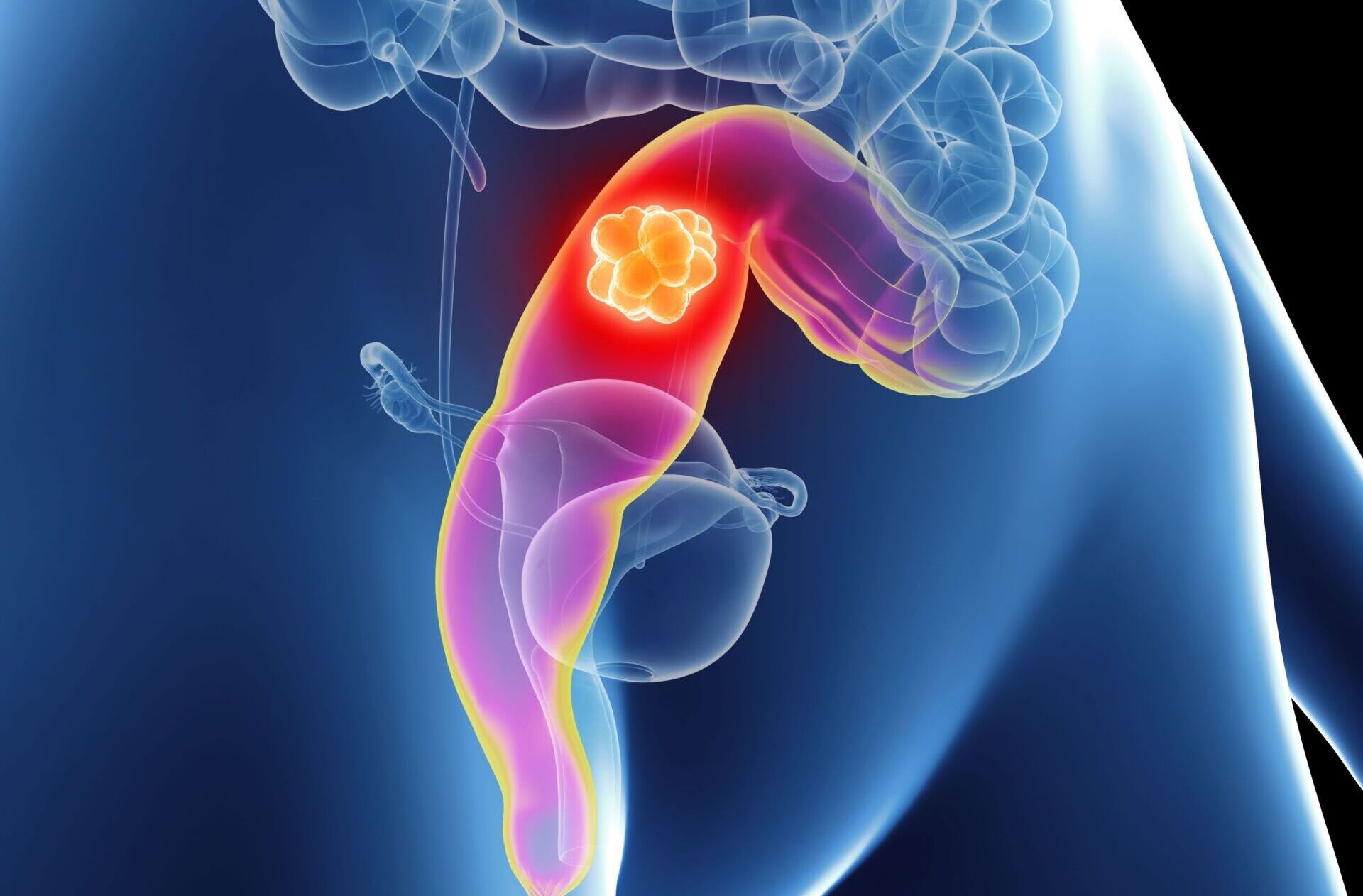
Almost always it is colon or rectal cancer (colorectal cancer), small bowel cancer is rare. In about one in five affected individuals, the tumor has already formed visible offshoots at the time of diagnosis (stage IV).
Colorectal cancer is more common on the left side of the bowel than on the right. The following is important for diagnosis and treatment: Most intestinal tumors, namely around 60 to 70 percent, are located in the last thirty centimeters of this organ: in the descending part of the colon, in the sigmoid or in the rectum.
Colon and rectal cancer almost always develop from (still benign) precursors that one day degenerate. These precursors are referred to as “polyps”, while the majority of them are adenomas, benign glandular growths. About one in five adenomas develops further in the course and can become dangerous. If adenomas are detected and removed in time, e.g. during a screening colonoscopy, up to 80 percent of colorectal carcinomas can be prevented.
If colorectal cancer is diagnosed, the type of therapy and also the chance of cure depend on many factors. The tumor stage is important, indicating how deeply the tumor has penetrated the intestinal wall, whether lymph nodes are affected and whether metastases are present. Each affected person is therefore examined closely and in detail.
Only a minority of colorectal tumors are detected at stage I, as symptoms almost never occur here. Most are not diagnosed until stage II or III. Then the cancer has already invaded all the walls of the intestine (stage II) or spread to adjacent lymph nodes (stage III).
Colorectal cancer can metastasize via the bloodstream, especially to the liver and lungs. Through the lymphatic vessels, the cancer cells primarily reach nearby lymph nodes and, by direct spread, the peritoneum. However, when viewed under the microscope, these metastases are similar in nature to the so-called primary tumor in the intestine from which they originally originated.
Colorectal Tumor Center
At the USZ, numerous departments have joined forces to form a colorectal tumor center. The center is certified according to the guidelines of the German Cancer Society (DKG). A team of experts specializing in the medical care of colorectal cancer works closely together here for the benefit of our patients. At DKG-certified centers, patients are treated according to strict quality criteria and, according to current studies, have a better chance of survival on average.
Colorectal cancer risk: what are the influencing factors?
Age, genes, environmental factors, intestinal polyps and chronic inflammatory bowel diseases such as ulcerative colitis or Crohn’s disease – these five risk factors can promote bowel cancer to a greater or lesser extent. The risk factor that usually weighs the most is age. From around the age of 50, the risk of developing the disease rises sharply until around the age of 80. However, colorectal cancer is also becoming more common in young people (<40-50 years), suspicious symptoms must be consistently clarified even in young adults.
One should be alert if adenomas appear before the age of 50. This is because the risk of colorectal cancer is then significantly higher not only for the affected person himself, but also for his parents and siblings. Adenomas that appear after the age of 60, on the other hand, are usually of no concern to relatives. Even if other cancers run in the family, such as stomach cancer or uterine cancer, it makes sense to discuss this with your doctor.
The likelihood of colorectal cancer increases more when several factors coincide. A healthy lifestyle can again reduce the risk.
According to the current state of knowledge, these influenceable factors include:
- little movement
- daily consumption of red meat (raw, dried, processed into sausage or fried)
- moderate to high alcohol consumption (two or more alcoholic drinks per day or more than about 60 grams of alcohol per week).
- Smoking
- Overweight, especially a lot of belly fat
- Low intake of dietary fiber (e.g., from cereals, legumes, fruits, and vegetables).
The best recipe against colorectal cancer is: enough exercise (preferably 30 to 60 minutes daily), reasonable body weight, healthy diet with sufficient fiber (preferably at least 30 grams daily), little alcohol and no smoking. This lifestyle statistically prevents about seven out of ten cases of colorectal cancer in men and four out of ten in women.
Colorectal cancer symptoms
The insidious thing about colorectal cancer is that these tumors usually grow “silently” for a long time, so those affected do not notice anything. When colorectal cancer becomes apparent, the tumor has often grown unnoticed for years. That’s why early detection screenings are so important.
Colorectal cancer can make itself felt with these symptoms:
- Changed bowel habits:
- Blood or mucus in or on the stool
- Diarrhea alternating with constipation
- newly appeared constipation
- Urge to defecate but no evacuation
- pencil thin stool
- tar black colored stool
- Anemia. The signs of anemia are fatigue, performance slump, skin pallor
- Recurrent abdominal pain and digestive problems
- Nausea, lack of appetite, feeling of fullness
- Weight loss even though you are not dieting
- Fever without signs of cold
Rarer signs:
- persistent itching in the anal area, for example if there is a tumor near the anus or the mucous membrane is irritated.
- recurrent aphthae in the mouth – especially in the case of advanced colon cancer, if the immune system is weakened or tumor therapy has been started. However, these are usually not directly related to the tumor itself, but occur concomitantly.
Of course, everyone has digestive problems at one time or another. But if they persist or recur, they should be taken seriously. See a doctor if you notice any warning signs of bowel cancer and don’t put off this consultation – it could save your life. Take a look in the toilet after every bowel movement. This means that you will notice any bleeding sooner, even if bowel cancer does not usually become noticeable for a long time.
Even though colorectal cancer is usually not noticeable for a long time. Nevertheless, both the precursors of the disease and colorectal cancer can be found with almost 100 percent certainty – provided that you look for them. This is what happens during “early detection.” Colorectal cancer screening is recommended in Switzerland for all individuals between 50 and 69 years of age. Risk groups (familial burden, chronic inflammatory bowel diseases) must be examined much earlier.
Second opinion colorectal cancer
When a cancer diagnosis is made, a second medical opinion is an important decision-making tool. The Comprehensive Cancer Center Zurich supports you with a professional expert opinion. They receive a thorough analysis of the situation as well as personal advice and quick answers to their questions.
What is the use of early detection?
Many of the bowel tumors that are discovered during a screening examination are still at an early stage and are easily treatable. Then the chance for a cure is high.
Two methods of screening are recommended for early detection in Switzerland: The blood-in-stool test and colonoscopy. These early detection methods provide the greatest benefit and are scientifically well tested.
In the view of many experts, there are very good arguments in favor of colonoscopy. Although the stool test for hidden blood is less burdensome, it is not very sensitive, especially in early stages and pre-stages, Colonoscopy is the method with the best overall track record. Any colon polyps can almost always be removed immediately during colonoscopy. In terms of cost, both screening methods are comparable over the years.
However, even the best early detection measure is of no use if it is not used regularly. Whichever one you choose: Get them done at the recommended intervals: Every two years for the fecal blood test and every ten years for the colonoscopy. If polyps have been found or if risk factors are present, the gastrointestinal specialist (gastroenterology) recommends closer monitoring.
Colorectal cancer screening
Of all the early detection measures, colonoscopy is the one with the best track record. It is currently recommended regularly from the age of 50.
Colorectal cancer stages: How advanced is the tumor?
When diagnosing colorectal cancer, the stage of the tumor is crucial. The stage describes how far the cancer has spread in the body – and is fundamental for the choice of therapy and the assessment of the chances of recovery.
Staging is based on the internationally recognized TNM classification:
- T stands for the tumor size or depth of spread into the intestinal wall
- N describes whether and how many lymph nodes are affected
- M indicates whether distant metastases are present (e.g. in the liver or lungs)
Colorectal cancer is then classified into the following stages:
- Stage 0 (carcinoma in situ): The cancer is still limited to the uppermost cell layer – a preliminary stage.
- Stage I: The tumor is limited to the intestinal mucosa or wall and has not affected any lymph nodes.
- Stage II: The tumor has grown further into the intestinal wall, but no lymph nodes are yet affected.
- Stage III: The tumor has spread to regional lymph nodes.
- Stage IV: There are distant metastases – e.g. in the liver or lungs.
How is colorectal cancer treated?
Treatment options for colorectal cancer are classically divided into three pillars:
- Surgery
- Radiotherapy
- Drug therapy/system therapy
To increase efficacy, several treatments are combined depending on the type, stage and spread of the colon tumor. The age and general condition of the affected person also play a role in the choice of therapies.
In many cases, surgery is a central component of treatment. The affected section of bowel is removed. Depending on the location and extent of the tumor, it may be necessary to temporarily or permanently create an artificial bowel outlet(stoma) – for example, if a direct connection of the remaining bowel sections is not possible or if the healing process is to be relieved.
The USZ specializes in state-of-the-art endoscopy and endoscopic tumor ablation, robotic minimally invasive surgery, innovative precision radiation, molecular oncology, immunotherapy and clinical trials. We offer forward-looking, multidisciplinary therapy concepts for the treatment of colorectal cancer according to the highest medical standards. We incorporate the latest scientific findings. An experienced team of experts from numerous disciplines is available to patients for consultation and treatment.
What are the chances of surviving bowel cancer?
Since around 1990, the prognosis for colorectal cancer has steadily improved, and this trend is currently continuing. In stage I, the disease can be cured in more than nine out of ten people affected. Survival rates for advanced colorectal cancer have also improved in recent decades.
Better and more early detection examinations have contributed to this, as have improved diagnostic methods, new surgical techniques, medications and other, new treatment methods. Switzerland is one of the countries with the highest survival rates for colorectal cancer.
Frequently asked questions about bowel cancer
Intestinal carcinoma often causes no symptoms at an early stage. However, the first signs of bowel cancer can be blood in the stool, persistent changes in bowel movements (such as diarrhea or constipation), abdominal pain, unwanted weight loss or fatigue. As these symptoms can also have other causes, medical clarification is important – especially from the age of 50 or if there is a family history.
In principle, the symptoms of bowel cancer can be similar in women and men. Nevertheless, in practice there are sometimes different focuses in the perception and severity of the complaints.
Colorectal cancer symptoms in women – frequently mentioned signs:
- Recurrent or diffuse abdominal pain
- Feeling of fullness or nausea without an identifiable cause
- Loss of appetite
- General exhaustion, which is often underestimated
Colorectal cancer symptoms in men – frequently mentioned signs:
- Blood in the stool or on the toilet paper
- Changed bowel habits (e.g. alternating between diarrhea and constipation)
- pencil thin stool
- unwanted weight loss
Important: These symptoms can occur in all genders. The decisive factor is not gender, but the duration and combination of symptoms. If they last longer or recur, a medical examination should be carried out – regardless of age or gender.
In Switzerland, bowel cancer screening is recommended from the age of 50 – or earlier if there is an increased risk (e.g. family history). Screening usually includes a colonoscopy, in which precancerous stages (polyps) can be detected and removed at an early stage. Alternatively, a stool test for hidden blood can be carried out – it is simple, but less reliable than a colonoscopy.
Bowel cancer usually develops over many years from benign growths in the bowel mucosa, known as bowel polyps. These precursors usually do not cause any symptoms, but can degenerate over time – i.e. become a malignant tumor. A colonoscopy allows polyps to be detected and removed at an early stage – often preventing the development of bowel cancer.
Certain blood values can be conspicuous in colorectal cancer, but are usually inconclusive. Anemia is often seen, for example due to a lack of iron – an indication of chronic blood loss in the intestine. Inflammatory values such as CRP or the tumor marker CEA (carcinoembryonic antigen) can also be elevated. However, CEA is more suitable for follow-up monitoring after diagnosis and not for early detection. A reliable diagnosis is only possible with further examinations – such as a colonoscopy.
Changes in stool color can be an indication of bowel cancer, but do not necessarily have to be. Visible blood in the stool is typical – this can then be reddish or dark in color (black), depending on where in the intestine the bleeding occurs. Very pale or pale stools can also be noticeable, but this is rather rare in bowel cancer. Important: Not every change means a serious illness – a medical check-up provides clarity.
The diagnosis is followed by careful clarification: How far has the cancer spread? Is an operation possible? The affected part of the bowel is usually surgically removed. Depending on the stage, chemotherapy or radiotherapy may also be necessary. The aim of the treatment is to completely remove the cancer and prevent it from recurring. During and after therapy, those affected are closely supported – both medically and psychologically.
Bowel cancer usually develops slowly – often over many years from benign polyps. When and whether it forms metastases depends on various factors: Tumor type, location, aggressiveness and individual factors. In the early stages, the cancer often remains localized. Early diagnosis significantly increases the chances of recovery and can prevent the cancer from spreading in the body.
If bowel cancer has already metastasized (e.g. in the liver or lungs), recovery is more difficult – but not impossible. In some cases, metastases can be surgically removed or controlled with modern therapies. The aim is then to reduce or even completely eliminate the cancer in the long term. Treatment is individually adapted and planned on an interdisciplinary basis, e.g. in one of the tumor boards at the University Hospital Zurich.
In around 5-10% of cases, bowel cancer is hereditary. The best known forms are Lynch syndrome and familial adenomatous polyposis (FAP). With these genetic diseases, the risk of developing bowel cancer at a young age is greatly increased. If you have several cases in your family or develop colorectal cancer at a very early age, you should seek genetic counseling.