





For patients
In the obesity consultation, we discuss individual diet and exercise measures and evaluate drug and surgical therapies.
Tel.
+41 43 254 04 44
Mail
azz@usz.ch
The USZ offers a world-class bariatric surgery program. Surgery can help to reduce weight in the long term and significantly reduce health risks.
Even in the era of GLP-1 agonists (weight loss injections), bariatric surgery continues to be of great importance, as it achieves significantly superior weight loss (approx. 65-75% of excess body weight), especially in the long term. After the procedure, many patients experience a considerable improvement in associated metabolic diseases and also a longer life expectancy. The very high patient safety of bariatric surgery has also been extensively studied and documented, so it is not surprising that bariatric surgery is now one of the most frequently performed operations.
Calculate BMIBariatric surgery reliably leads to weight loss and also reduces the risk of many diseases, such as:
At the USZ, the Roux-Y gastric bypass and sleeve gastrectomy are the main procedures performed; depending on the individual situation, other procedures may also be considered.
Sleeve gastrectomy (gastric sleeve surgery) and gastric bypass are by far the most important surgical procedures, accounting for around 90% of all bariatric procedures performed worldwide.
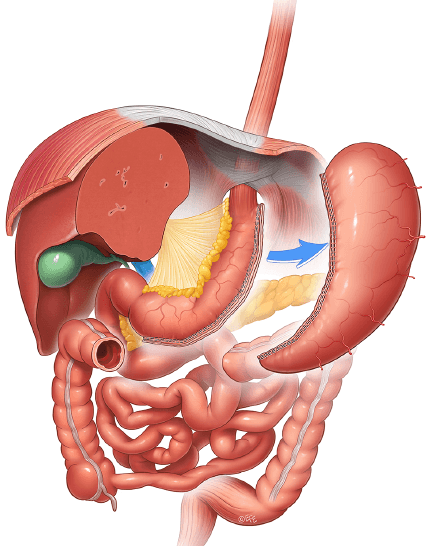
© Dr Levent Efe, courtesy of IFSO
In this minimally invasive procedure, around 80% of the stomach is removed through small incisions in the skin. What remains is a “tubular stomach” with a diameter of two to three centimeters, which leads to faster gastric emptying and thus to earlier satiety. As a result, patients reduce the portion size per meal, which leads to rapid weight loss and long-term maintenance of the achieved weight level. In addition, the production of the so-called hunger hormone (ghrelin), which is mainly produced in the gastric fundus, is significantly reduced. The results in terms of weight loss over 10 years are comparable to those of gastric bypass. The duration of gastric sleeve surgery is shorter than with gastric bypass and long-term nutritional deficits occur less frequently, although long-term weight loss is somewhat lower and gastroesophageal reflux is somewhat more common. It can also be performed as the first step of a two-phase bariatric approach when conversion to gastric bypass is required for inadequate weight loss, secondary weight gain or persistent gastroesophageal reflux disease.
Gastric bypass surgery is one of the most established bariatric methods for achieving significant weight loss and alleviating associated diseases. This is a minimally invasive procedure in which a small stomach pouch is formed which absorbs the ingested food and transports it to the small intestine via a new connection (shown in yellow in the image).
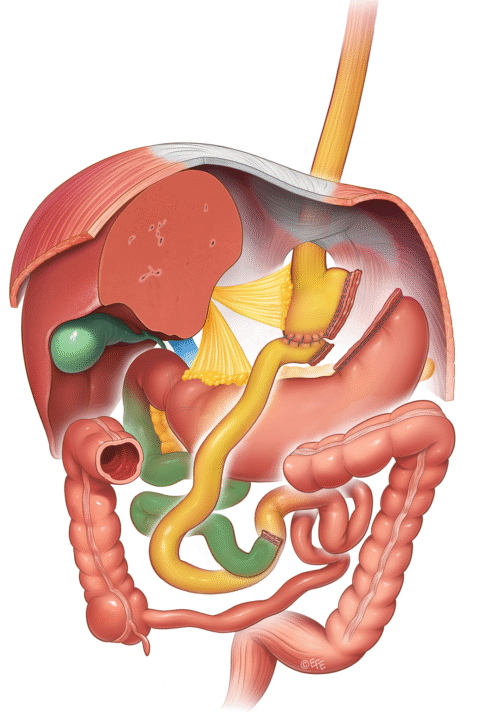
© Dr Levent Efe, courtesy of IFSO
The secretions produced in the remaining (excluded) stomach and the digestive juices of the bile and pancreas (shown in green in the image) mix with the food at a more distant point in the small intestine, which is then digested in the common channel to the large intestine. In contrast to gastric sleeve surgery, no part of the gastrointestinal tract is removed. The operation leads to rapid gastric emptying and thus to rapid satiety and a reduction in portion size. This results in a reduced calorie intake with rapid weight loss and very good weight maintenance. The operation leads to reduced absorption of some vitamins and trace elements, which must therefore be replaced and regularly monitored for the rest of the patient’s life.
The first step is to clarify whether weight loss surgery is an option for you. If there are no concerns, further clarifications will follow:
In some cases, the following additional examinations may be necessary:
It can take between 2-4 months to carry out the above-mentioned clarifications. At the USZ, we offer patients a comprehensive assessment during a short hospital stay in order to shorten the process.
Follow-up examinations are an important part of the treatment concept. In addition to monitoring weight progression and nutrition adapted to the operation, it serves to detect and prevent deficiencies at an early stage. Regular blood tests are carried out to determine whether certain vitamins or minerals need to be supplemented. Pregnancy should be avoided in the first period (approx. 18-24 months) after the operation.
The follow-up examinations initially take place every 3-6 months. If the treatment progresses well, they can be reduced to annual checks after 24 months. However, our team is available 24 hours a day in case of problems. If necessary, we also offer the full range of revision surgeries following previous bariatric surgery, including treatment of weight gain, hiatal hernia/reflux, excessive weight loss, chronic pain (internal hernia, intussusception, gastric banding issues, etc.) or severe dumping syndrome.
All cases are discussed weekly in our interdisciplinary “Obesity Board” and thus receive 360-degree input from all health experts involved.
Large excess skin is often present after significant weight loss. These are usually located in the hip, breast, buttock or thigh area. This may require one or more surgical procedures to remove or tighten skin tissue. Unfortunately, these body contouring operations are not always covered by health insurance. The decision on cost coverage depends more on somatic factors than on aesthetic reasons.
Tummy tuck offerIf indicated, bariatric surgery is a mandatory benefit covered by health insurance, so it is not necessary to submit a cost approval application to a certified center. The detailed guidelines for this can be found at www.smob.ch. The most important criteria are:
In many cases, bariatric surgery can create the conditions for other medical treatments to be carried out safely and successfully. At the USZ, we therefore work closely with highly specialized departments and have developed structured clinical pathways for the following situations:
Joint replacement operations: Hip or knee replacements are associated with increased risks in patients who are very overweight. Prior weight loss through bariatric surgery can improve the chances of success of these procedures.
Abdominal wall hernias: Obesity increases the risk of large hernias, complications during surgery and recurrence. Prior obesity treatment can significantly improve the surgical conditions.
Treatment of abdominal wall hernias
Organ transplants: Being severely overweight can affect suitability for a liver, kidney, heart or lung transplant. Weight reduction through bariatric surgery can help to restore the ability to transplant.
Offer kidney disease
Treatment of liver cirrhosis
Pregnancy with PCOS: In women with polycystic ovary syndrome, bariatric surgery can have a positive effect not only on weight but also on hormonal disorders and increase the chances of pregnancy. PCOS Center
Idiopathic intracranial hypertension: Studies show that weight reduction after bariatric surgery can significantly reduce intracranial pressure – a decisive factor in the treatment of this rare disease. To the offer
In the obesity consultation, we discuss individual diet and exercise measures and evaluate drug and surgical therapies.
Leading experts in the field of obesity from a wide range of disciplines work closely together to define a customized treatment pathway for your patients. We look forward to your assignment.
After a gastric bypass or gastric sleeve operation, a special diet is followed. On the first day after the operation, we start to build up your diet. One day of clear liquid, followed by 2 days of liquid food, 2 days of finely pureed food and then another 2-3 weeks of soft food. From about 3-4 weeks onwards, you can slowly switch to a normal diet.
In principle, the following applies:
Yes. Especially after gastric bypass surgery, you must continue with vitamin and mineral supplementation to avoid nutritional deficiencies. These deficiencies can be caused by reduced intake and difficulty absorbing nutrients after the procedure. There is also a risk of developing a disease caused by a long-term nutritional deficiency (e.g. osteoporosis). Most patients need a multivitamin preparation, calcium (approx. 1200 mg), iron for menstruating women (325 mg) and vitamin B12 (one injection per 3 months). Vitamins can be taken in tablet or liquid form. If you opt for a multivitamin tablet, take one in the form of a chewable tablet or a multivitamin for children. Do not take calcium and iron minerals together and try to avoid taking vitamins on an empty stomach.
In our experience, the majority of patients who have undergone gastric bypass or gastric sleeve surgery have reduced their excess weight by 50% after 6-9 months. The weight curve usually stabilizes after about 12-18 months.
The extent to which large excess skin flaps form depends on a person’s tissue type, the extent of weight loss and their age. If these skin flaps cause chronic irritation and infections, so-called fat apron operations can be covered by health insurance. The costs for this must be applied for from the health insurance company. The plastic surgeon will help with the application process. Health insurance companies usually make the assumption of costs dependent on the existence of health problems or a limited ability to work.
The side effects vary in their occurrence and extent and are difficult to predict. Some people report problems such as diarrhea, increased wind shedding and vomiting. Most side effects can be reduced by changing the composition of your diet. Malnutrition is rare with the current interventions, although vitamin/mineral supplementation is extremely important. All patients must take certain supplements for the rest of their lives, as the operation causes changes in the absorption of nutrients and reduced fluid intake.
This varies from person to person and depends on the procedure. Every postoperative complication understandably leads to a longer stay for the patient. On average, without complications after surgery, the stay for a laparascopic gastric bypass or sleeve gastrectomy is around 2-3 days. Patients can usually return to work 3-4 weeks after the operation.
The costs of surgery and the associated costs for anesthesia, hospitalization, medication, etc. are covered by health insurance if